

Submitted by BLampkins_CSTE on
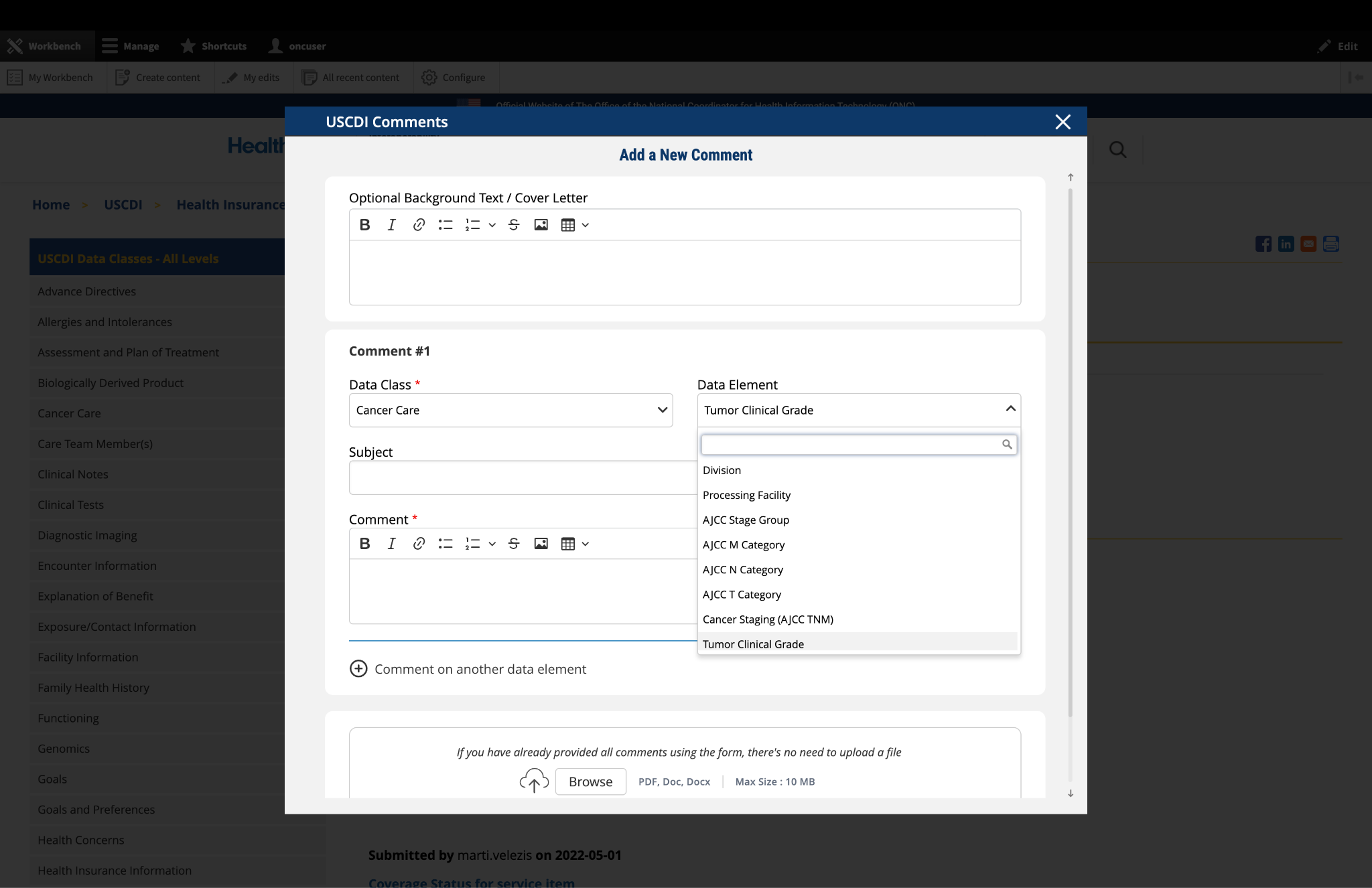
Specimen Collection Date/Time - CSTE Comment
| CSTE supports collection of more granular laboratory data to support case adjudication and reporting as well as patient deduplication and linking of data from cases to ELR, which can be critical. The variables we recommend be added to USCDI v7 include: Name of testing/performing laboratory and associated identifiers (CLIA)(HIGH PRIORITY) Name of ordering provider and submitter Address of testing/performing laboratory Accession number at testing laboratory (HIGH PRIORITY for matching purposes) Date the test was ordered Date the test was performed (needs to be reconciled with results date/timestamp) Specimen collection date and time (HIGH PRIORITY) (Needs to be reconciled with Test Date=Clinically relevant time) Test result value (needs to be reconciled with values/results in USCDI V1 and V2), units, reference range and interpretation (HIGH PRIORITY) Abnormal flag (HIGH PRIORITY) Test kit identifier Dates and times are critical to evaluating the timeliness of reporting - it is a major indicator for the performance of public health surveillance systems and without this information it is unknown how data exchange is impacting the ability for public health to respond in a timely fashion. Although the date and time data are generated by the system, in practice it has been observed that availability of this data to Public Health Departments is sparse for use in timeliness analysis |
Submitted by minigrrl on
What is the justification…
What is the justification for the demotion of the following Case Reporting data elements in USCDI, specifically:
• Exposure/Contact Information: Exposure/Contact Agent
• Exposure/Contact Information: Exposure/Contact Date
• Exposure/Contact Information: Exposure/Contact Direction
• Exposure/Contact Information: Exposure/Contact Source/Target Participant
• Exposure/Contact Information: Exposure/Contact Type
• Health Insurance Information: Medicare Patient Identifier
• Immunizations: Vaccination Administration Date
• Laboratory: Specimen Collection Date/Time
• Patient Demographics/Information: Patient Birth Place
• Patient Demographics/Information: Tribal Enrollment
• Pregnancy Information: Estimated Date of Delivery
• Pregnancy Information: Gestational Age
• Pregnancy Information: Last Menstrual Period (LMP)
• Provenance: Unique Identifier
• Social Determinants of Health: Housing Instability and Homelessness
• Social History: Congregate Living
• Work Information: Employment Status
• Work Information: Job Employer Address
• Work Information: Job Employer Name
• Work Information: Usual Industry
• Work Information: Usual Occupation
Currently, 21 certified EHR products exchange these elements using electronic Case Reporting (eCR) specifications demonstrating real-world adoption that typically supports promotion, not demotion, within the USCDI maturity model.
Collectively, these elements provide clinical, demographic, occupational, social, and epidemiological context essential to disease investigation and outbreak response for nationally notifiable conditions.
We urge ONC to either reverse this decision or publish a detailed, evidence-based rationale.