Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Submitted By: Michelle Dougherty
/ Submitted on behalf of the CMS Data Element Library (DEL) Health IT Workgroup
Data Element Information
Data Element Description
This data element carries information on Mental Functioning that is exchanged as observations. (Observations are characteristics that can be tested, measured, or observed and are communicated with a name-value pair structure). Mental functioning is a broad domain. Using the conceptual framework of the International Classification of Function (ICF), it includes aspects such as memory functions, orientation functions, attention functions, etc.
Notes:
• This data element is constrained to health data represented in data structures for observations. Observations should be represented using terminologies supporting this conceptual model, such as LOINC, which is designed for this purpose. Representing problems, goals, and other types of information related to functioning should use other data class structures as appropriate.
• Examples of Mental function concepts can be found in the ICF browser at: https://apps.who.int/classifications/icfbrowser
• Examples of demonstrated use of Mental Function data can be found in the PACIO FHIR Cognitive Function Implementation Guide which supports exchange of observation data from PHQ-9, BIMS, CAM, MOCA, MMSE assessments coded with LOINC.
Use Case Description(s)
Use Case Description
Exchange of Data for Transitions of Care and Care Coordination:
Data exchange between acute care, post-acute care (PAC) providers, the patient and caregivers, and other care settings (physician practices, community based services, etc.), using common standards and definitions, supports patient-centered care by providing access to longitudinal information at transition and facilitating care coordination. An ASPE and CMS study found that 45% of Medicare patients required PAC services after an acute hospital stay.* The importance of exchanging data elements related to functioning at transition of care is described in the findings of the 2020 national study on hospital adoption of electronic health record functionality to support age-friendly care.** It concluded that US acute care hospital EHRs lack key features and health information exchange of important information that supports care for older adults, including structured documentation on mentation and mobility. Emerging work on frailty indices have found relationships between poor physical functioning and risk of adverse health outcomes.*** An ASPE funded project is currently exploring how health systems may use EHR-based data for frailty algorithms, including aspects of frailty related to mobility and cognitive limitations. Having functional limitations does not necessarily mean that a person is frail. Widespread exchange of the content specified in this data class (and corresponding data elements) proposal has the potential to improve patient and provider communications and supports access to longitudinal information that enables improved efficiencies, improved quality of care, and improved health outcomes.
The 2014 Improving Medicare Post-Acute Care Transformation (IMPACT) Act required the standardization and interoperability of specific categories of PAC patient assessment content, including the content applicable to the proposed data elements. For PAC settings including SNFs, HHAs, and specialty hospitals (inpatient rehabilitation facilities (IRFs), long term care hospitals (LTCH)), standardized patient assessment data reported to the Centers for Medicare and Medicaid Services (CMS) includes items about mental function, mobility, self-care and domestic life/IADLs that represented as observations. All of these concepts are represented in LOINC. The conceptual framework of the International Classification of Functioning (ICF) informed the development of these and other functioning data elements. Prior to use on the patient assessment, these data elements were tested for validity and reliability and are used for quality measurement, payment, public reporting and oversight.
Representation of functioning observations is well supported by all of the common exchange paradigms, including messages, documents, and APIs. Here we highlight the two most prevalent.
• FHIR: The HL7 PACIO project is focused on advancing interoperable health data exchange between PAC and other providers, patients, and key stakeholders across health care. The project has developed a FHIR Functional Status Implementation Guide and a FHIR Cognitive Status Implementation Guide (IG) which will be balloted as a standard for trial use in October 2020. The IG leverages the FHIR exchange structures and LOINC-coded observations. Successful exchange of functioning data from PAC assessments using the PACIO IGs was demonstrated in the January, May, and September 2020 Connectathons. PAC assessment data about mental function, mobility, self-care, and domestic life/IADLs are also included in use cases for the eLTSS and Care Plan HL7 FHIR projects.
• C-CDA: This data class and data elements are aligned with C-CDA templates for mental status and functional status. Functioning information from SNF and HHA patient assessments are being exchanged with HIEs and other providers using HL7 C-CDA. This exchange is supported by select EHR vendors, VorroConnect KeyHIE Transform, and the 360X data exchange initiative.
Sources:
*RTI International analysis of 2014 Medicare claims under contract with the Assistant secretary for Planning and Evaluation, August 2018, unpublished
**Hospital adoption of electronic health record functions to support age-friendly care: results from a national study. JAMIA 08/2020. https://pubmed.ncbi.nlm.nih.gov/32772089/
*** Validation of a Claims-Based Frailty Index Against Physician Performance and Adverse Health Outcomes in Health and Retirement Study. J Gerontol A Biol Sci Med Sci, 2019, Vol. 74, No. 8, 1271–1276
- VorroConnect: https://vorroconnect.com/products/healthcare-information-exchange/
- 360X: https://oncprojectracking.healthit.gov/wiki/display/TechLab360X/360X+Home
Estimate the breadth of applicability of the use case(s) for this data element
Stakeholder estimates can be challenging since the proposed data elements should be usable across the continuum of care, and beyond the traditional healthcare system – into the community. We know that PAC providers are required to collect standardized and interoperable data elements related to functioning at patient admission, discharge, and specified time intervals using defined CMS assessments. However, standardized capture of data elements related to functioning is inconsistent in other healthcare settings such as acute care hospitals and primary care/specialty care physician practices.
In attempting to quantify stakeholders potentially involved in the use and exchange of data elements related to functioning, we relied on the July 2020 CMS Fast Facts to provide a picture of both providers and patients (i.e., beneficiaries), albeit from a Medicare perspective. While the numbers that appear below are significant, it is important to remember that they are constrained to Medicare providers and persons served who are covered by original Medicare. Non-Medicare providers and patients who are not covered by original Medicare (e.g., Medicaid only, privately insured, etc.) are not reflected in the counts but would still be stakeholders for the proposed data elements. It is also important to note that caregivers and providers of long term supports and services (e.g., home health aides, meals on wheels) are increasingly recognized as important stakeholders in health information exchange but are also not reflected in the metrics below.
Institutional Medicare Providers (for 2019) & Persons Served (original Medicare for 2018)
• Inpatient Hospitals - 6,023 providers; 6.5 million persons served
• SNFs - 15,103 providers; 1.7 million persons served
• HHAs – 11,157 providers; 3.6 million persons served (Medicare Part A skilled and Medicare Part B non-skilled services)
Notes:
• The CMS Fast Facts reports include the 306 IRF providers and 367 LTCH providers, who are subject to CMS PAC assessment provisions, in the “inpatient hospital” counts for both providers and persons served. There is no setting specific count of persons served for these IRF and LTCH providers.
• Other types of Medicare Institutional providers were identified that would be stakeholders for data elements related to functioning, but for which separate counts of persons served were not available. There were 21,000+ providers identified as outpatient physical therapy/speech pathology, rural health clinics, federally qualified health centers, comprehensive outpatient rehab facilities, or hospice providers.
Non-institutional Medicare Providers (for 2019)
• Primary care, surgical specialties, medical specialties, and psychiatry – 537,390 providers
• Non-physician practitioners – 489,765 providers
Note:
• The non-physician practitioner classification (e.g., nurse practitioners, physician assistants) does not provide sufficient detail to discern the numbers of these practitioners associated with the targeted primary care and specialty providers.
Support Quality Measures:
Standardized and interoperable PAC functioning data elements have the potential to be utilized to support clinical quality measures (CQMs) in a variety of existing quality reporting programs and future digital quality measures.
• Mental Status: As cognitive function can impact patient safety, as well as overall physical functioning, the data elements could be used for a quality measure that is focused specifically on cognition but may also be relevant to the construct of other eCQMs. Currently, CMS149v8, Dementia: Cognitive Assessment, has been validated for use with nursing home patients only using the Minimum Data Set (MDS) Brief Interview of Mental Status (BIMS).
• Mobility, Self-care, Domestic Life/IADLs: Dependence on others for ADL assistance can lead patient’s to feelings of helplessness, isolation, diminished self-worth, and loss of control over one’s destiny. As inactivity increases, complications such as pressure ulcers, falls, contractures, depression, and muscle wasting may occur.
• Functioning data elements could be used for a quality measure that is focused specifically on this data element (e.g., MIPS CQM #282: Dementia: Functional Status Assessment), and may also be relevant to the construct of other eCQMs. The Clinical Reasoning and PACIO FHIR initiatives have used PAC data in the May and September 2020 Connectathon demonstrations of CMS149 and CMS104.
Currently, there are six NQF endorsed measures that address concepts of functioning (NQF #2631 thru 2636) and use standardized data elements related to functioning from PAC assessments. One or more of these NQF measures are a component of the CMS Quality Reporting Programs (QRPs) for SNFs, IRFs, LTCHs, and HHAs. Additionally, data related to functioning are used in quality measures that help inform facility ratings in the Five Star Quality Rating System whose results are made available on CMS public reporting websites.
Estimate the breadth of applicability of the use case(s) for this data element
Stakeholder estimates can be challenging since the proposed data elements should be usable across the continuum of care, and beyond the traditional healthcare system – into the community. We know that PAC providers are required to collect standardized and interoperable data elements related to functioning at patient admission, discharge, and specified time intervals using defined CMS assessments. However, standardized capture of data elements related to functioning is inconsistent in other healthcare settings such as acute care hospitals and primary care/specialty care physician practices.
In attempting to quantify stakeholders potentially involved in the use and exchange of data elements related to functioning, we relied on the July 2020 CMS Fast Facts to provide a picture of both providers and patients (i.e., beneficiaries), albeit from a Medicare perspective. While the numbers that appear below are significant, it is important to remember that they are constrained to Medicare providers and original Medicare persons served. Non-Medicare providers and patients who are not covered by original Medicare (e.g., Medicaid only, privately insured, etc.) are not reflected in the counts but would still be stakeholders for the proposed data elements. It is also important to note that caregivers and providers of long term supports and services (e.g., home health aides, meals on wheels) are increasingly recognized as important stakeholders in health information exchange but are also not reflected in the metrics below.
Institutional Medicare Providers (for 2019) & Persons Served (original Medicare for 2018)
• Inpatient Hospitals - 6,023 providers; 6.5 million persons served
• SNFs - 15,103 providers; 1.7 million persons served
• HHAs – 11,157 providers; 3.6 million persons served (Medicare Part A skilled and Medicare Part B non-skilled services)
Notes:
• The CMS Fast Facts reports include the 306 IRF providers and 367 LTCH providers, who are subject to CMS PAC assessment provisions, in the “inpatient hospital” counts for both providers and persons served. There is no separate count of persons served for these IRF and LTCH providers.
• Other types of Medicare Institutional providers were identified that would be stakeholders for data elements related to functioning, but for which separate counts of persons served were not available. There were a were 21,000+ providers identified as outpatient physical therapy/speech pathology, rural health clinics, federally qualified health centers, comprehensive outpatient rehab facilities, or hospice providers.
Non-institutional Medicare Providers (for 2019)
• Primary care, surgical specialties, medical specialties, and psychiatry – 537,390 providers
• Non-physician practitioners – 489,765 providers
Note:
• The non-physician practitioner classification (e.g., nurse practitioners, physician assistants) does not provide sufficient detail to discern the numbers of these practitioners associated with the targeted primary care and specialty providers.
Improving patient experience of care (quality and/or satisfaction)
Improving the health of populations
Reducing the cost of care
Improving provider experience of care
Maturity of Use and Technical Specifications for Data Element
Applicable Standard(s)
LOINC.
LOINC is a freely available global standard that contains a well-developed model for representing variables, answer lists, and the collections that contain them.* Many clinical assessments, scales, and other observations related to functioning are present in LOINC, including all of the variables on the PAC assessments for SNFs, IRFs, LTCHs, and HHAs. Regenstrief operates a robust process for adding new content (including functioning assessment instruments) if key gaps are identified.
*PMID: 22899966
PACIO Project: FHIR Cognitive Status Implementation Guide (STU ballot scheduled for October 2020)
PACIO Project: FHIR Functional Status Implementation Guide (STU ballot scheduled for October 2020)
Current Use
In limited use in test environments only
Extent of exchange
N/A
Potential Challenges
Restrictions on Standardization (e.g. proprietary code)
We are not aware of restrictions on standardization of proposed data elements in PAC settings. However, we are not aware of standardization of these proposed data elements in other care settings such as acute care hospitals, physician practices, etc.
Restrictions on Use (e.g. licensing, user fees)
Intellectual property issues related to use of the BIMS, CAM, and PHQ2/PHQ9 in PAC assessments have been addressed through appropriate annotations on printed and electronic representation of these items. as proposed data elements have not been standardized in acute care settings, assessments of functioning used in these settings would need to be evaluated for intellectual property considerations.
Privacy and Security Concerns
This data should be exchanged securely. Secure data transfer process as governed by CMS and ONC should be followed
Estimate of Overall Burden
PAC settings such as SNFs, IRFs, LTCH, and HHAs, are required to report standardized patient assessment data to CMS for purposes of Medicare payment, quality reporting, and compliance surveys. These patient assessments include concepts of mental function, mobility, self-care and domestic life/IADLs.
Outside of the post-acute care settings, these data elements may not be structured and are not captured with consistency.
Other Implementation Challenges
For PAC settings, the proposed data elements are collected from standardized assessments and reported to CMS using agency specific data submission protocols and specifications. However, as PAC providers are excluded from EHR certification requirements, there is significant variance in the adoption of interoperability terminologies and exchange standards by EHR vendors supporting post-acute care settings. Additionally, while some providers may capture mental status, mobility, self-care and/or domestic life/IADL data in acute care or outpatient settings, they may use other instruments (observations) to capture this data.
On behalf of the American Speech-Language-Hearing Association (ASHA), I write to share ASHA’s support of PACIO's recommendation to add the International Classification of Functioning, Disability and Health (ICF) as an Applicable Vocabulary Standard. ASHA is the national professional, scientific, and credentialing association for 247,000 members, certificate holders, and affiliates who are audiologists; speech-language pathologists (SLPs); speech, language, and hearing scientists; audiology and speech-language pathology assistants; and students. Audiologists specialize in preventing and assessing hearing and balance disorders as well as providing audiologic treatment, including hearing aids. SLPs identify, assess, and treat speech, language, swallowing, and cognitive communication disorders.
Recommendation: Add the International Classification of Functioning, Disability and Health (ICF) as an Applicable Vocabulary Standard to the Functional Status, Health Concerns, and Mental/Cognitive Status data elements.
Rationale: The PACIO Project Community* recommends the addition of the World Health Organization’s International Classification of Functioning, Disability and Health (ICF) as an Applicable Vocabulary Standard to the Health Concerndata element.
Background: The ICF was created in 2001 to classify functioning domains as a consequence of health conditions, which are not completely captured by any other codeable concept ontology. The ICF ontology allows data to be categorized as mental, cognitive, and functional factors, as well as health concerns in a machine-readable way.
The WHO developed the ICF to be ICD complementary, with ICF covering functioning and environmental factors and ICD covering diseases and other health problems. As described by the WHO, “ICF is based on the same foundation as ICD…and share the same set of extension codes that enable documentation at a higher level of detail.”
The PACIO Project makes extensive use of the ICF ontology in the Personal and Functional Engagement (PFE) FHIR IG STU-2 as category codes for several profiles.
Current Standards
Current Use
All post-acute care (PAC) vendors can collect data pertaining to Functional Status and Mental/Cognitive Status given CMS requirements to collect such data required for PAC facilities to get reimbursement (e.g., Minimum Data Set for nursing facilities, Inpatient Rehabilitation Facility Patient Assessment Instrument [IRF-PAI]); therefore, all vendors have the potential to apply ICF to the volume of Functional Status and Mental/Cognitive Status data already collected.
Three vendors have deployed the PACIO PFE IG that integrates the ICF: Global Alliant, Open City Labs, and Patient Centric Solutions.
Current Exchange
The ICF-integrated PACIO PFE IG has been used to successfully exchange ICF-coded data during the July 2025 CMS Connectathon applied to the PHQ-9 assessment and January 2026 HL7 Conenctathon applied to the PROMIS-10 measure.
On behalf of the American Speech-Language-Hearing Association (ASHA), I write to share ASHA’s support of PACIO's recommendation to Expand the definitions of Functional Status and Mental/Cognitive Statusdata elements to include the American Speech-Language-Hearing Association (ASHA)Functional Communication Measures (FCMs) that have assigned LOINC codes . ASHA is the national professional, scientific, and credentialing association for 247,000 members, certificate holders, and affiliates who are audiologists; speech-language pathologists (SLPs); speech, language, and hearing scientists; audiology and speech-language pathology assistants; and students. Audiologists specialize in preventing and assessing hearing and balance disorders as well as providing audiologic treatment, including hearing aids. SLPs identify, assess, and treat speech, language, swallowing, and cognitive communication disorders. The services provided by ASHA members are medically necessary, evidence-based, and essential to the health and independence of Medicaid beneficiaries across the lifespan.
Recommendation: Expand the definitions of Functional Status and Mental/Cognitive Statusdata elements to include the American Speech-Language-Hearing Association (ASHA)Functional Communication Measures (FCMs) that have assigned LOINC codes.
Rationale: The PACIO Project Community* recommends including Functional Communication Measures (FCMs), in the definitions of the Functional Status and Mental/Cognitive Status data elements to demonstrate the capability in each of these domains for capturing communication specific health information. Inclusion of FCMs would help support patient- and caregiver-centered care as well as patient engagement.
Current Standards
Background: FCMs were created by the American Speech-Language-Hearing Association (ASHA) and are is “used to describe an individual’s functional abilities over the course of speech-language pathology intervention in a given level of care,” according to an ASHA user guide. Eight FCMs have been endorsed by NQF for use in the Physician Quality Reporting System, including: Attention, Memory, Motor Speech, Reading, Spoken Language Comprehension, Spoken Language Expression, Swallowing, and Writing. Of note, an NQF-endorsed measure “tends to be one that is generally regarded as a high-quality measure” by CMS.
Technical: LOINC includes FCM items, organized within a swallowing panel (99852-6), cognition panel (99788-2), Multi-Modal Functional Communication panel (99828-6), Spoken Language Comprehension panel (99836-9), and Spoken Language Expression panel (99844-3).
Current Use
Practice: The FCMs are the discipline standard for speech, language, and hearing assessments and are included in the National Outcomes Measurement System (NOMS). The purpose is to support longitudinal collection of speech, language, and hearing data to inform clinical care and support quality service provision (ASHA).
Technical: There is a NOMS "SMART on FHIR" app for Epic and Cerner Customers that supports collection of FCM data (NOMS includes FCM items).
Current Exchange
The NOMS is available via a “SMART on FHIR” app for Epic and Cerner Customers also supports transmission of FCM data via its inclusion in NOMS.
The FCM data are captured under both Functional Status and Cognitive Status as part of a published PACIO Personal and Functional Engagement (PFE) FHIR IG STU-2, compliant with US Core 6.1.0.
Breadth of Applicability
FCM data are collected by clinicians, including Speech Language Pathologists (SPLs) and audiologists, across various care settings, including post-acute care settings (ASHA). The FCM is not a required to be collected, but is collected by these specialties to support care (example of FCM usage available via ASHA NOMS data reports for 671,628 adults and 3,967 children ages 3-5).
FCM data can be electronically submitted to the NOMS system by participating organizations that integrate NOMS into their EHR systems.
Applicable standards: The PACIO Community recommends including FCMs within the Functional Status and Mental/Cognitive Status data elements.
The proposed USCDI data elements related to the exchange of data for transitions of care and care coordination can significantly enhance electronic Patient-Reported Outcomes (ePRO) enablement, including other eCOAs (electronic Clinical Outcome Assessments), by ensuring that critical functional status and cognitive assessments are seamlessly integrated into care workflows. By standardizing the exchange of data between acute care providers, post-acute care (PAC) settings, and patients, these elements facilitate access to comprehensive longitudinal information, which is vital for effective patient engagement and decision-making. The focus on mental function, mobility, and self-care—concepts represented in LOINC and supported by FHIR and C-CDA standards—ensures that patients and caregivers can report on their functional status accurately and consistently. This alignment promotes better communication between healthcare providers and patients, leading to improved care coordination and quality. Moreover, the incorporation of validated and reliable data elements into PAC assessments supports the development of frailty algorithms, allowing for more personalized care approaches and potentially reducing adverse health outcomes. Overall, enhancing ePRO capabilities through these standardized data exchanges not only improves efficiency but also contributes to better health outcomes for patients, particularly older adults requiring coordinated care across multiple settings.
The overall classification of Health Status Assessments (HSAs) can significantly enhance ePRO and other digital methods for gathering clinical data from patients, caregivers, and practitioners. For instance, the FHIR IG for Structure Data Capture (SDC), which utilizes Questionnaire and QuestionnaireResponse resources, can streamline the collection of forms related to existing HSAs, including Functional Status, Mental/Cognitive Status, Pregnancy Status, Alcohol Use, Substance Use, and Physical Activity Status. Many of these assessments are not only integral to clinical care but are also highly prescriptive within the context of clinical research. For example, a clinical trial protocol may cite various HSAs or comparable questionnaires as outlined in the Schedule of Activities (see https://hl7.org/fhir/uv/vulcan-schedule/STU1/). In other use cases, they may be structured for their use in RWE by way of RWD sources (see https://hl7.org/fhir/uv/vulcan-rwd/STU1/).
HL7 recommends that Depression Assessment listed under Health Status Assessment as an example screening of interest, recognizing that not all health information technology (HIT) may need to support that when being certified. Depressive disorders are common mental disorders that occur in people of all ages. Major depressive disorder (MDD) is the second leading cause of disability worldwide, affecting an estimated 120 million people. Depression has a large effect on health care costs and on productivity. Adolescents with depression have higher medical expenditures, including those related to general and mental health care, than adolescents without depression. For working-adults, one study showed a relationship between the severity of depression symptoms and work function and found that for every 1-point increase in a Patient Health Questionnaire 9 (PHQ-9) score (a measure of depression severity); patients experienced an additional mean productivity loss of 1.65%. Even minor levels of depression symptoms were associated with decreases in work function. The U.S. Preventive Services Task Force (USPSTF) recommends screening for depression among adolescents 12-18 years and the general adult population, including pregnant and postpartum women.
Health Status – Mental Function / Mental Health Status and Cognitive Status
NACHC supports the separation of the current "Mental/Cognitive Status" element into two distinct components: "Mental Health Status" and "Cognitive Status". While these elements naturally fall under the broader category of "Health Status Assessment", it is crucial to recognize their unique clinical nature and definitions. "Cognitive Status" is assessed using established measures like MoCA, SLUMS, or MMSE, evaluating orientation, attention, memory, judgment, and reasoning. In contrast, "Mental Health Status" encompasses diagnoses such as depression, anxiety, and ADHD, and is evaluated using validated assessments like PHQ-9, GAD-7, and the Vanderbilt Assessment Scale. NACHC encourages ONC to support work on a list of preferred instruments and mappings that will assist organizations in normalizing these types of data.
The urgency of this matter is underscored by staggering statistics from the Centers for Disease Control and Prevention (CDC). Over 50% of individuals in the United States will receive a mental health diagnosis in their lifetime, with more than 57 million annual visits to physician offices where mental disorders are the primary diagnosis. Additionally, the U.S. Preventive Services Task Force (USPSTF) has recommended depression screening for various populations since 2016, extending to adolescents, children, and pregnant or postpartum women as of 2022.
Furthermore, the National Committee for Quality Assurance (NCQA) places a high priority on the diagnosis of depression due to its well-documented impact on physical health, mental health, and functional status. This commitment led to the development of five depression care measures within the Healthcare Effectiveness Data and Information Set (HEDIS), notably focusing on the PHQ-9 assessment tool.
We believe that implementing these recommendations will significantly enhance the comprehensive assessment of mental health, leading to more effective care and improved patient outcomes.
Data Elements: Functional Status, Mental/Cognitive Status, Disability Status (Draft V4)
Recommendation: Remove the Disability Status data element from the Health Status data class and instead add a new data element entitled, “Disability” to the patient demographic data class.
Rationale: The PACIO (Post-Acute Care Interoperability) Project, established February 2019, is a collaborative effort between industry, government, and other stakeholders, with the goal of establishing a framework for the development of FHIR implementation guides to facilitate health information exchange. The PACIO Community supports CMS and CDC submission, which reflect their view that identifying a person with a disability does not necessarily have any bearing on how healthy a person is or the status of one’s health. However, collecting and transmitting data on disability in a standardized way alongside other demographic factors is vital to recognition of disability as a key component of identity and allows analysis of outcomes and conditions in an intersectional way, incorporating race/ethnicity, age, sex, and disability together for a more comprehensive understanding of patient demographics.
Data Elements: Functional Status, Mental/Cognitive Status, Disability Status (Draft V4)
Recommendation: Adopt the value sets developed for the “Personal Functioning and Engagement” IG as part of the USCDI V3 updates to the U.S. Core IG to incorporate Functional Status and Cognitive Status data elements.
Rationale: The PACIO (Post-Acute Care Interoperability) Project, established February 2019, is a collaborative effort between industry, government, and other stakeholders, with the goal of establishing a framework for the development of FHIR implementation guides to facilitate health information exchange. Functional and Mental/Cognitive Status are important data classes that have widespread use in all healthcare settings and sharing the content of standardized PAC assessments (some of which are federally required) with non-PAC providers (e.g., hospitals, physicians) would improve the quality of care and facilitate care coordination during transitions of care. These instruments use a consistent framework mapped to HIT standards for functional status, contain administrative and clinical patient data, can be considered as individual data elements (mobility, pressure ulcer, transportation, social isolation, etc.) or a “questionnaire” of grouped data elements together (MDS, OASIS, IRFPAI, FASI etc.) The PACIO Community wishes to update the ONC/USCDI with current efforts relating to several of the data elements under the proposed USCDI V4 data class of Health Status (Health Concerns, Functional Status, Disability Status, and Mental/Cognitive Status). The PACIO Community recognized the value of creating data models (like Gravity’s SDOH) that allow for expansion across multiple domains. As a result, PACIO created a new FHIR Implementation Guide (IG), “Personal Functioning and Engagement,” which consolidates PACIO’s prior published IGs (STU1) “Cognitive Status” and “Functional Status”. The PACIO group also is incorporating data elements of communication, swallowing, and hearing to the “Personal Functioning and Engagement” IG currently under development. Currently, the Personal Functioning and Engagement IG data structures focus on observation/ assessment data. However, the IG could include future expansion using additional resources as the work matures. The concept of “Personal Functioning and Engagement” encompasses both an individual’s abilities (positive strengths) and disabilities (impairments) across all types of functioning. The PACIO Community examined and incorporated the International Classification of Functioning, Disability and Health (ICF) as a conceptual framework that underpins this new PACIO Personal Functioning and Engagement IG. PACIO’s current work focuses on ICF “Body Functions” including mental functions, sensory functions (including hearing), voice and speech functions, and ingestion functions (swallowing). Current PACIO focus for ICF “Activities and Participation” functions include Learning and Applying Knowledge, Communication, Mobility, and Self-care.
In the USCDI v.3, the definition of Cognitive Status does not mention worsening/better whereas the functioning definition does. The current definition of Functional Status (“Assessment of a patient’s capabilities, or their risks of development or worsening of a condition or problem. (e.g., fall risk, pressure ulcer risk, alcohol use)" is includes the capabilities (positive aspect of functioning) and the risk for worsening (negative aspect of functioning). This may be confusing to the user.
The PACIO Community recommends the adoption of the International Classification of Functioning, Disability, and Health (ICF) conceptualization of functioning. The ICF defines functioning as the positive or neutral aspects of the interrelationships of the person, their health condition, and contextual factors (personal and environmental factors). This definition would provide a uniform approach to the definitions of disability and functional status. In addition, if adopting the ICF framework, Functional Status and Cognitive Status would consider positive or neutral aspects of their domain as the definition of both use the term “functioning.” However, if ONC retains the existing definition of functioning, for consistency, the PACIO Community recommends including worsening/better in the Cognitive Status definition for USCDI v.4.
To maximize the utility of the data exchanged during transitions of care, the PACIO Community recommends including the questions and answers, expressed using LOINC, for the Functional and Mental/Cognitive Status data elements that are part of the federally required PAC assessment instruments, not just what functional or Mental/Cognitive assessment was performed.
The American Occupational Therapy Association supports and appreciates the inclusion of mental functions in the health status data class. AOTA participates in the PACIO Project work on the Cognitive Status Implementation Guide that has since been renamed to Functional Performance. Developing an interoperable and interdisciplinary method of collecting information on an individual's mental functions is crucial in early detection of cognitive decline, onset of delirium, or identification of trends over time. AOTA encourages ONC to consider how this data can be efficiently and accurately collected beyond admission and discharge and how data from other clinicians, such as occupational therapy practitioners, can be utilized in this data class.
NACHC is supportive of the concept of mental function; however, it is not likely to support interoperability to solely create a terminology binding to support the concept. Because the concepts in the draft version generally represent non-semantically equivalent types of cognitive function and observations about these conditions, we believe that creating a class for this concept will likely create larger transitions of care documents without being able to be processed by receiving systems.
Furthermore, there will likely be confusion between which assessments constitute “Functional Status” and “Mental Function”. Would recommend renaming this term. This approach creates liability for providers who at best can use this data as free text in this case and contributes to data overload and burnout.
We strongly recommend providing either specific categories of functional status with equivalent semantics and clear terminology bindings.
The "Optional Background Text / Cover Letter" field provides space for additional context or introductory information related to your comment.
If you wish to provide context, explanation, or an introduction to your comment, enter this information in the field labeled "Optional Background Text / Cover Letter." This is entirely optional and is most useful when submitting multiple related comments or when additional background would help reviewers understand your feedback.
If you are only commenting on a single data class or element, you may leave this field blank.
2. Select the Data Class
To specify which data class your comment addresses:
In the "Data Class" drop-down menu, select the appropriate data class you want to comment on.
If you are providing a general comment that is not specific to a data element, select "General" from the options. Comments with this designation will be displayed on the USCDI landing page.
Note that the Data Class field will automatically populate based on your current location in the platform:
If you are on a data class page, the field will be set to that specific data class
If you are on a data element page, the corresponding data class will be pre-selected
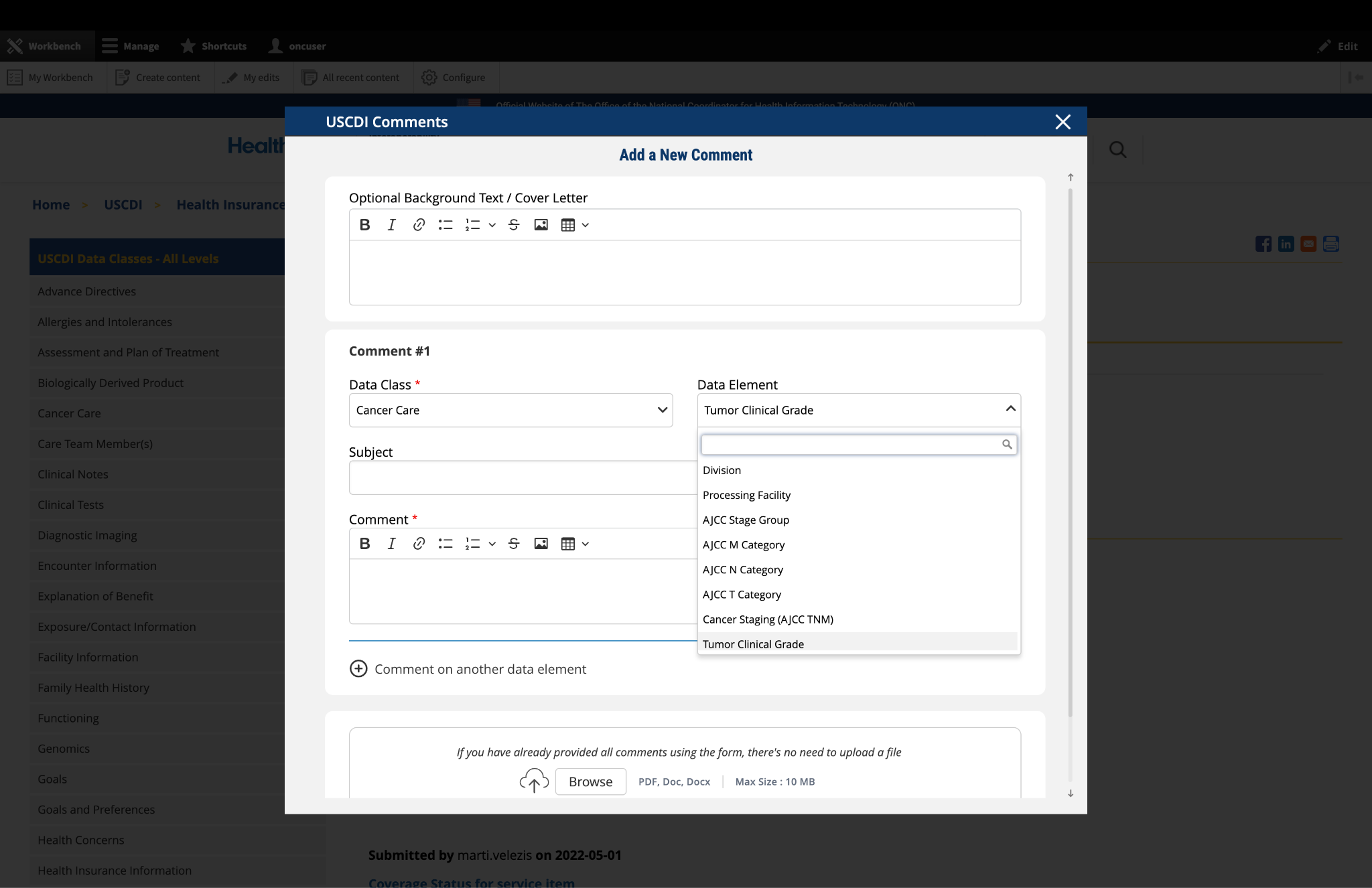
3. Select the Data Element
To specify which data element your comment addresses:
In the "Data Element" drop-down menu, select the specific data element you want to comment on.
The drop-down menu will display only the elements available under the data class you selected in the previous step.
You can use the search function within the drop-down to quickly locate a specific data element.
If you are commenting on the data class itself rather than a specific element, you may leave this field blank.
Note: Comments on a specific data element will appear on the respective data element page, while comments on a data class (without a specific element selected) will appear on the landing page for that data class.
Fig 1 The "Data Class" and "Data Element" dropdown menus allow users to specify the exact content they wish to comment on.
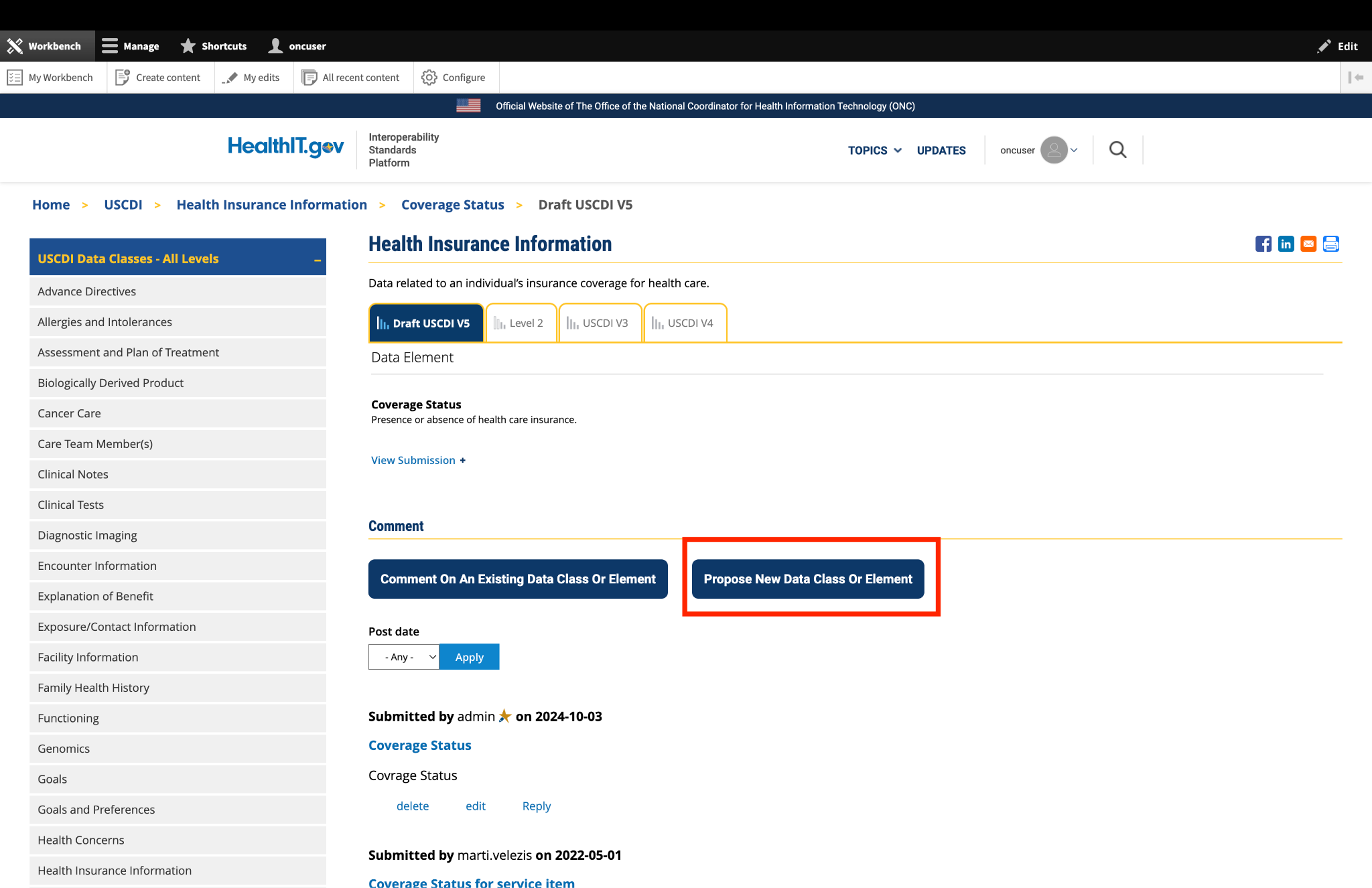
4. Optional: Propose New Data Class or Element
If you cannot find the appropriate data class or element for your comment:
Instead of clicking the "Comment On An Existing Data Class Or Element" button, click the adjacent button labeled "Propose a New Data Class or Data Element."
This will redirect you to the ONDEC (ONC New Data Element and Class) Submission System.
In the ONDEC system, follow the provided instructions to submit your proposal for a new data class or element.
Once your proposal is submitted through ONDEC, it will be reviewed separately from the commenting process.
Fig 2 The "Propose a New Data Class or Data Element" button redirects users to the ONDEC Submission System for proposing new data elements not currently available in the system.
5. Complete the Comment Form
Fill out the required fields in the comment form:
Subject: Enter a brief, descriptive title that summarizes your comment. This helps reviewers quickly understand the nature of your feedback.
Comment: In this field, provide the full details of your comment or feedback. Be as clear and specific as possible about your suggestions, concerns, or observations. Include any relevant details that support your position.
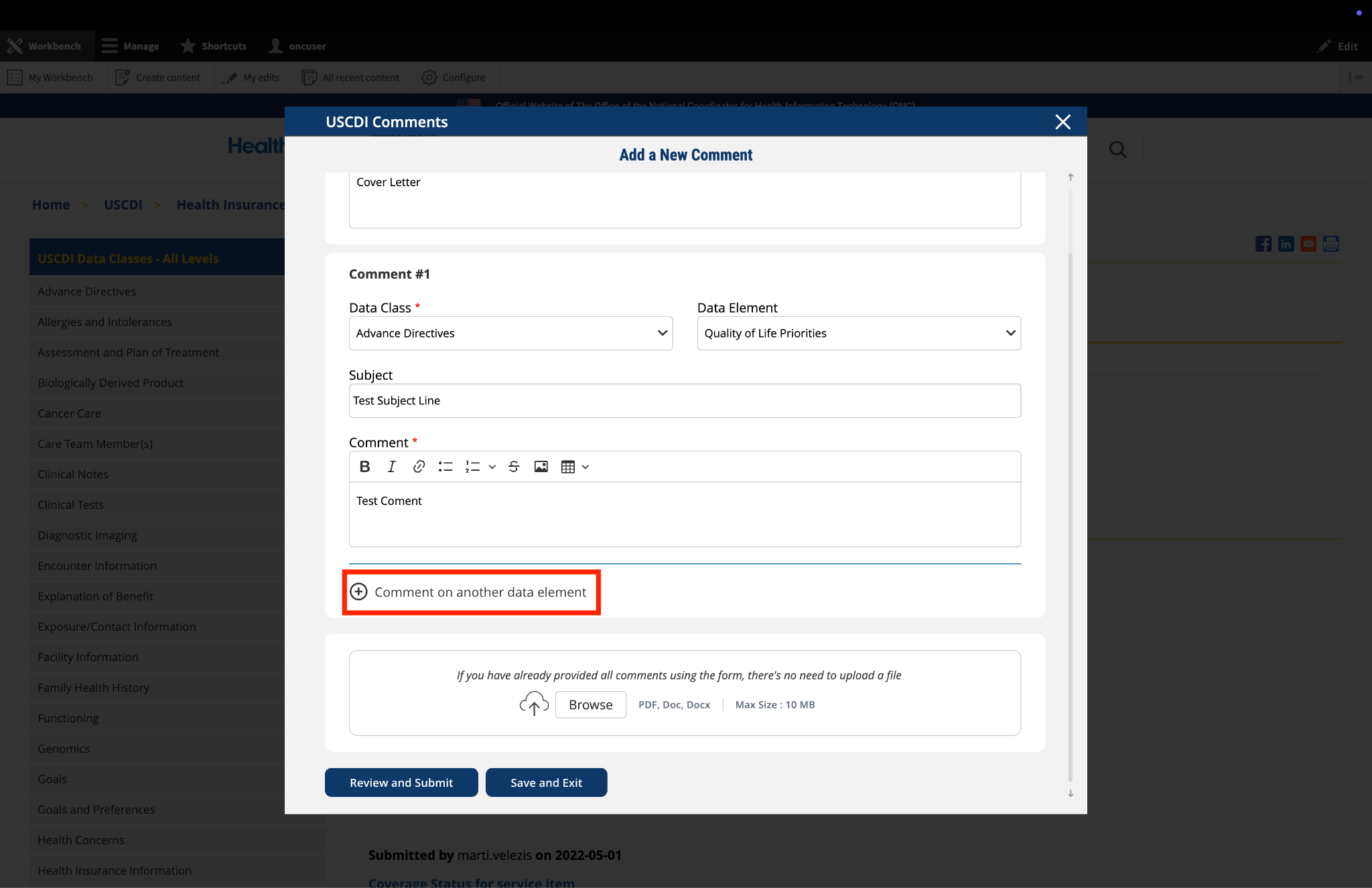
6. Optional: Add Additional Comments
If you need to comment on multiple data classes or elements:
After completing your first comment, click the link labeled "Comment on another data element" at the bottom of the form.
A new comment section will appear, allowing you to enter details for your additional comment.
For each additional comment, you must select the appropriate data class and data element from the drop-down menus.
Complete the Subject and Comment fields for your additional comment.
Repeat this process for each additional comment you wish to submit.
Fig 3 The "Comment on another data element" link enables users to create multiple comments addressing different elements within a single submission.
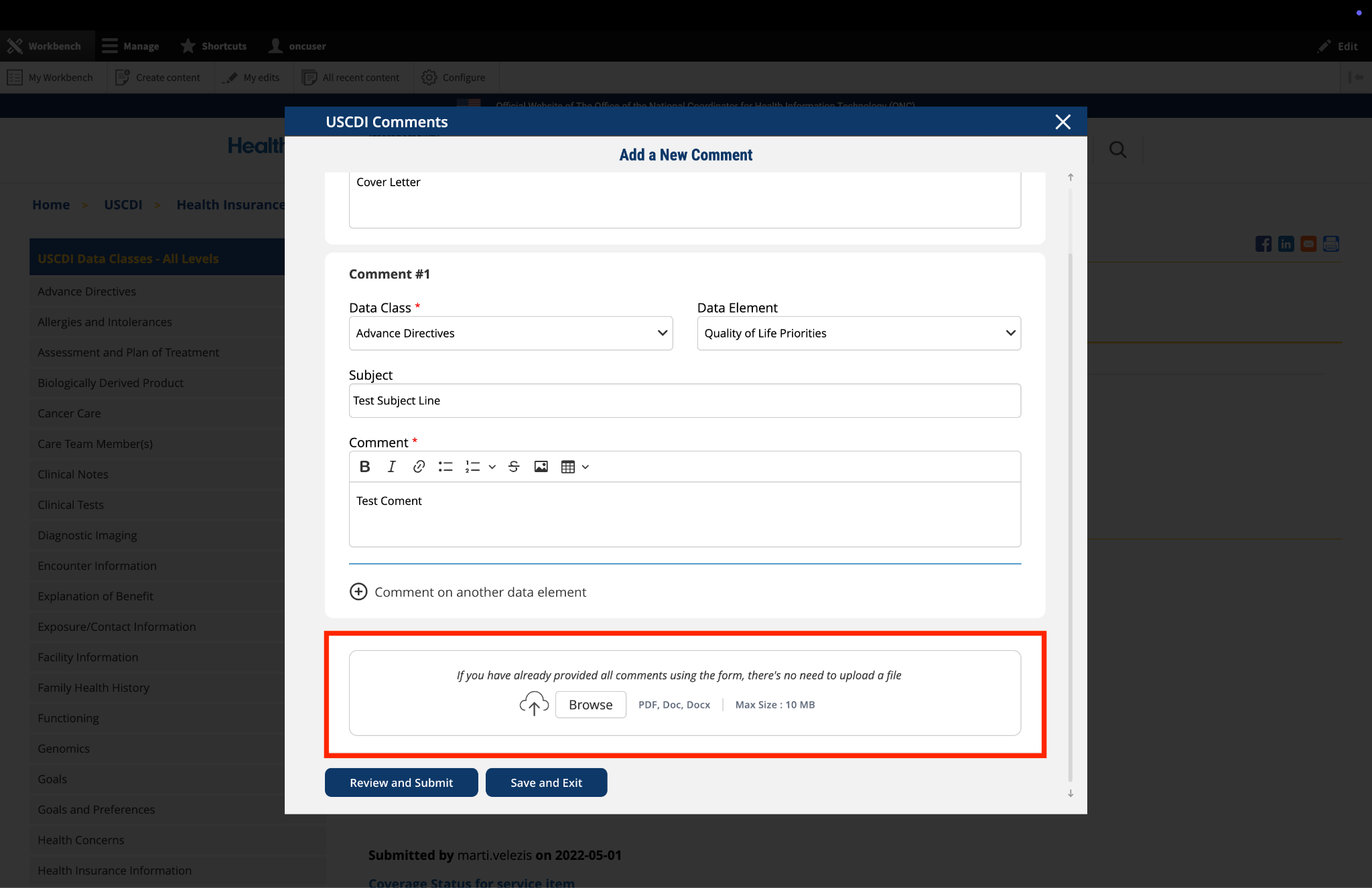
7. Optional: Upload Supporting Files
The platform allows you to upload supporting documentation to enhance your comment:
Locate the "File Upload" section at the bottom of the comment form.
Click to upload any files (such as PDFs or documents) that provide additional context, evidence, or clarification for your comment.
Important: If you have already entered your comments using the form fields, there is no need to upload duplicate content in PDF format. The file upload feature is intended for supplementary materials only. Please avoid uploading files that contain the same information already provided in your comment text.
Fig 4 The "File Upload" section permits users to attach supporting documentation that supplements their written comments.
8. Optional: Save and Exit
If you need to pause your work and return to complete your comment later:
Click the "Save and Exit" button at the bottom of the form.
Your comment will be saved as a draft that you can access and complete later.
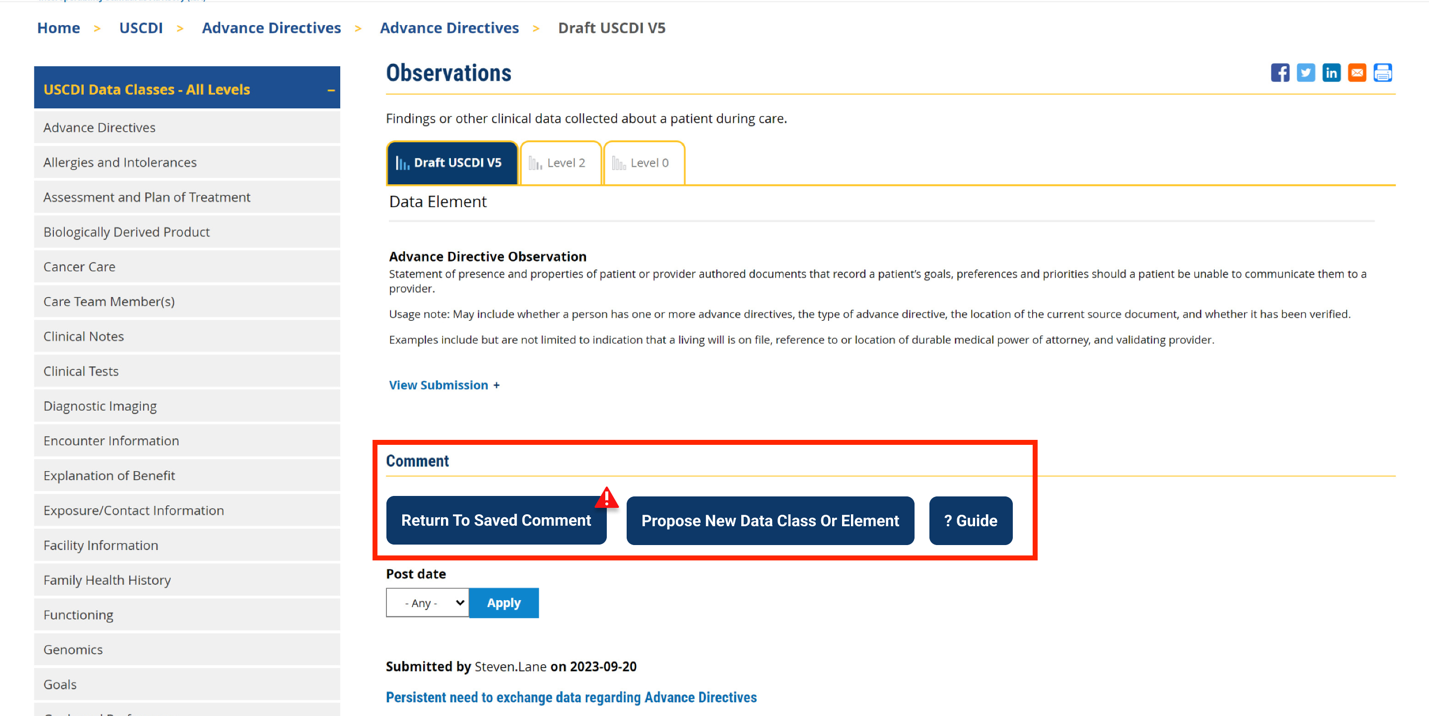
When you return to the platform, you will see a red triangle with an exclamation mark next to the “Return to saved Comment” button, indicating that you have saved comments in draft status.
Click this button to continue working on your draft.
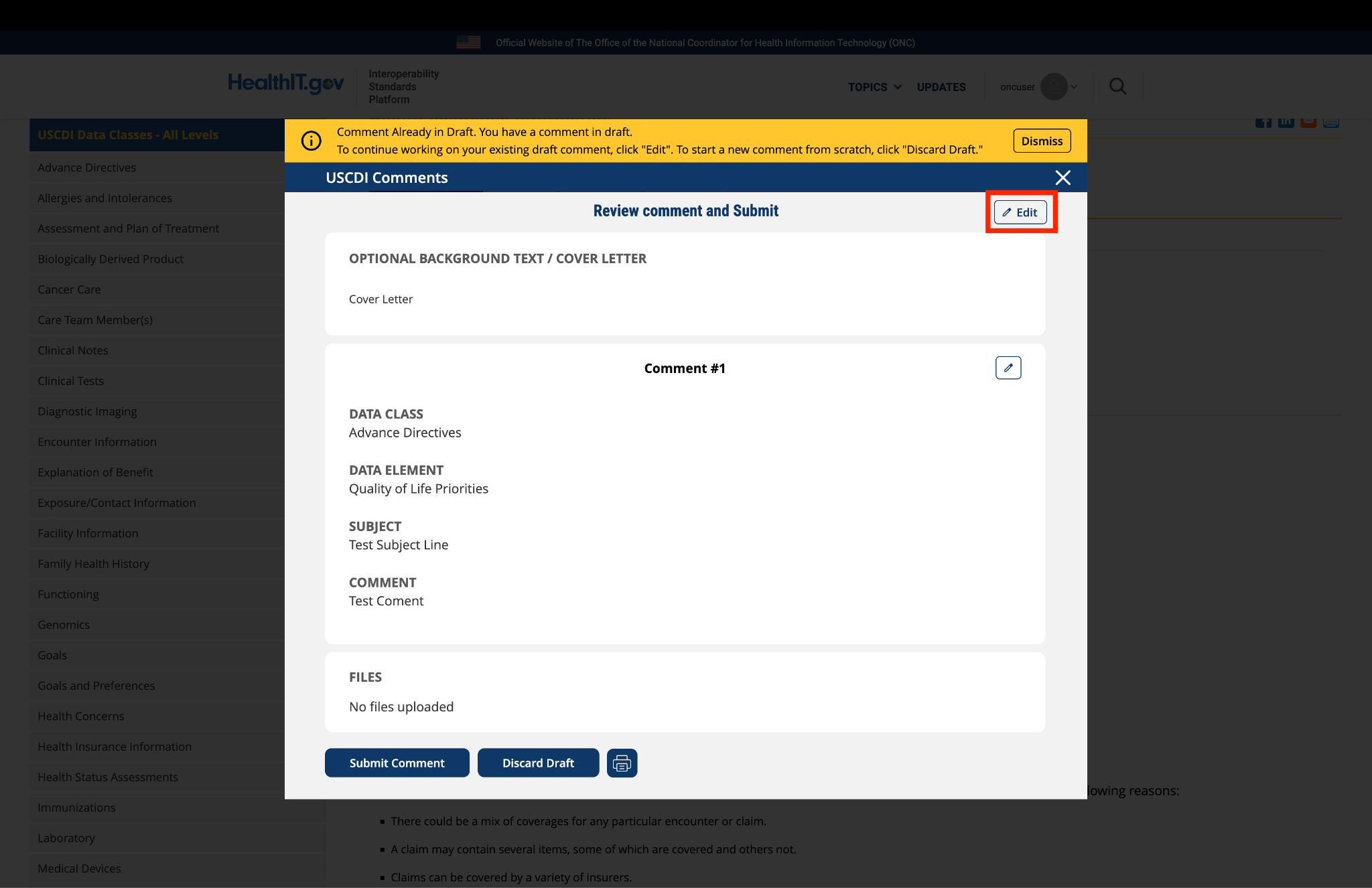
You will be taken to a review page where you can:
Select "Submit Comment" to officially submit your feedback.
Click "Edit" to return to the comment form and make changes
Select "Discard Draft" to delete the saved draft and start fresh
Fig 5 A red triangle with exclamation mark indicator appears next to the “Return to saved Comment” button when draft comments are saved in the system.
9. Review and Submit
Once you have completed your comment:
Click the "Review and Submit" button at the bottom of the form.
This will take you to a review screen displaying your comment(s) in full.
Review all information for accuracy and completeness.
On this review screen, you have three options:
Click "Submit Comment" to officially submit your feedback
Click "Edit" to return to the comment form and make changes
Click "Discard Draft" to delete the comment and start fresh
The review screen also includes a "Print" button that allows you to create a printed copy of your comments for your records.
If you choose to submit, your comment will be recorded in the system and made available for review by the appropriate stakeholders.
Fig 6 The review screen allows users to verify comment content and make any necessary modifications before final submission.


Submitted by RebeccaB on
ASHA: Add ICF as an Applicable Vocabulary Standard
On behalf of the American Speech-Language-Hearing Association (ASHA), I write to share ASHA’s support of PACIO's recommendation to add the International Classification of Functioning, Disability and Health (ICF) as an Applicable Vocabulary Standard. ASHA is the national professional, scientific, and credentialing association for 247,000 members, certificate holders, and affiliates who are audiologists; speech-language pathologists (SLPs); speech, language, and hearing scientists; audiology and speech-language pathology assistants; and students. Audiologists specialize in preventing and assessing hearing and balance disorders as well as providing audiologic treatment, including hearing aids. SLPs identify, assess, and treat speech, language, swallowing, and cognitive communication disorders.
Recommendation: Add the International Classification of Functioning, Disability and Health (ICF) as an Applicable Vocabulary Standard to the Functional Status, Health Concerns, and Mental/Cognitive Status data elements.
Rationale: The PACIO Project Community* recommends the addition of the World Health Organization’s International Classification of Functioning, Disability and Health (ICF) as an Applicable Vocabulary Standard to the Health Concern data element.
Current Standards
Current Use
Current Exchange