Provides information or details regarding modifications, tools, technologies, and/or other supports needed in order to address any barriers to care that an individual living with a disability(ies) may need in order to improve their care and life with a diagnosis.
Use Case Description(s)
Use Case Description
Individuals living with disabilities face barriers to receiving proper medical care when their doctors and care teams are not aware of existing disabilities. Consequently, these barriers exacerbate health disparities and result in inferior care and poor outcomes. Appointments may need to be rescheduled, care may not be coordinated properly, breakdowns in communication and trust will also negatively impact patient care without carefully documenting disability status. If properly documented, an alert could notify appropriate care team members and staff to address any physical access barriers, arrange for interpreters, plan for various forms of communication and patient support tools.
Applications for disability benefits could be further automated and streamlined with the addition of this data element.
If we are going to improve the lives and care of individuals living with disabilities, we must prioritize capturing and sharing this data accordingly.
Estimate the breadth of applicability of the use case(s) for this data element
SNOMED International recommends that ONC designate SNOMED CT U.S. Edition as an applicable vocabulary standard for the Accommodations data element.
SNOMED CT physical object and clinical finding hierarchies include a validated range of concepts relevant to accommodation documentation by covering assistive devices (hearing aids, mobility aids, communication devices), disability-related modifications, and care access requirements. This supports the health equity objectives of the ONC Health IT Certification Program and aligns with federal accommodation requirements under Section 504 of the Rehabilitation Act and the Americans with Disabilities Act.
SNOMED International recommends that ONC consider a complementary dual designation of SNOMED CT (for clinical concept coding of specific accommodations) and LOINC (for observation and questionnaire structure), consistent with the established complementary roles these standards play across multiple USCDI data classes. This approach aligns with HL7 FHIR US Core, where LOINC codes identify observation types and SNOMED CT codes identify clinical values. A dual designation would also ensure Accommodations data can be represented in both structured clinical documentation and patient-facing questionnaire formats, supporting the CMS Interoperability and Patient Access Final Rule's requirements for patient access to their own health data.
Recommendation: The PACIO Project Community* recommends updating the data element description for Accommodations to include legal caregivers or representatives of the patient, who are also covered by law to receive accommodations.
Suggested Data Element Description: Modifications, tools, technologies, and other supports necessary to access care by the patient and their companions.
Rationale
Healthcare organizations are already collecting accommodation data, but are doing so in a non-standardized way, according to a 2024 study published in the Journal on Quality and Patient Safety.
There are several federal regulations that require accommodations be provided to parents/caregivers with disabilities, often called “companions” within the regulations, either because they are specifically called out in the regulation or because the regulations are broad and can be applied to parents/caregivers.
Regulations specific to parents/caregivers include:
Title II of the Americans with Disabilities Act (ADA) (28 C.F.R.) § 35.160(a) states that “A public entity shall take appropriate steps to ensure that communications with applicants, participants, members of the public, and companions with disabilities are as effective as communications with others…For purposes of this section, ‘companion’ means a family member, friend, or associate of an individual seeking access to a service, program, or activity of a public entity, who, along with such individual, is an appropriate person with whom the public entity should communicate.” This definition includes “an appropriate person” which necessarily encompasses legal guardians, conservators, and healthcare proxy holders.
ADA § 36.303(c) identifies companions with disabilities as the people receiving accommodations: “A public accommodation shall furnish appropriate auxiliary aids and services where necessary to ensure effective communication with individuals with disabilities. This includes an obligation to provide effective communication to companions who are individuals with disabilities.” The Department of Justice provided guidance for this section that specifically calls out that often “covered entities communicate with someone other than the person who is receiving their goods or services”; the rules “require covered entities to provide effective communication for companions who have communication disabilities.”
Regulations that require accommodations for those with disabilities in general, which can be applied to caregivers/parents:
Title II of the Americans with Disabilities Act (ADA) and Section 504 of the Rehabilitation Act “provides that no qualified individual with a disability shall, by reason of such disability, be excluded from participation in or be denied the benefits of the services, programs, or activities of any entity that receives Federal financial assistance, or be subjected to discrimination by such entity.”
Title 28 § 36.303 requires that “public accommodation shall take those steps that may be necessary to ensure that no individual with a disability is excluded, denied services, segregated or otherwise treated differently than other individuals because of the absence of auxiliary aids and services, unless the public accommodation can demonstrate that taking those steps would fundamentally alter the nature of the goods, services, facilities, privileges, advantages, or accommodations being offered or would result in an undue burden, i.e., significant difficulty or expense.”
Affordable Care Act (ACA) Section 1557 (42 U.S.C. §18116) part 92, §92.1 regarding nondiscrimination in health programs or activities “prohibits discrimination on the basis of race, color, national origin, sex, age, and disabilityin certain health programs and activities. Section 1557 provides that, except as otherwise provided in title I of the ACA, an individual shall not, on the grounds prohibited under title VI of the Civil Rights Act of 1964, title IX of the Education Amendments of 1972, the Age Discrimination Act of 1975, or section 504 of the Rehabilitation Act of 1973, be excluded from participation in, be denied the benefits of, or be subjected to discrimination under, any health program or activity, any part of which is receiving Federal financial assistance, including credits, subsidies, or contracts of insurance, or under any program or activity that is administered by an executive agency or any entity established under title I of the ACA. This part applies to health programs or activities administered by recipients of Federal financial assistance from the Department, Department-administered health programs or activities, and title I entities that administer health programs or activities.”
* The PACIO (Post-Acute Care Interoperability) Project, established February 2019, is a collaborative effort between industry, government, and other stakeholders, that aims to advance interoperable health information exchange between post-acute care (PAC) providers, patients, and other key stakeholders across health care.
As a disability/health scholar and social work professional who co-chairs the WHO Functioning and Disability Reference Group, I strongly support the recommendation to move Accommodation from Level 0 to Level 2.
Patients with chronic health and mental health conditions often require accommodations across diverse health and social care settings in order to access high quality, equitable health care services. Accommodations reduce health disparities by removing the disabling structural and functional barriers that prevent them from accessing services and participating fully in their own care.
When patients' needs are met and preferences are respected through accommodation, it leads to greater safety and overall satisfaction with their healthcare experience. Satisfied patients are more likely to adhere to treatment plans, follow medical advice, and take medications as prescribed. This leads to better health outcomes and reduced healthcare costs.
I write in agreement with the comments of the Post-Acute Care InterOperability (PACIO) Project, the Disability Equity Collaborative, the Disability Health Equity Research Network, and Centers for Medicare & Medicaid Services (CMS) that the Accommodation data element should be advanced from Level 0 to at least Level 2. As PACIO’s comments document, Accommodation data are already represented by several well-vetted and well-used terminology standards, including LOINC. They are already captured by multiple EHRs from multiple vendors, including Epic and Cerner. Accommodation data apply broadly across health care settings and use cases for over 70 million adults (over 28 percent) in the United States with a disability. CMS's comments document that federal programs are exchanging Accommodation data, but even if the current level of exchange is uncertain notwithstanding broad capability, need, and use, no doubt that reflects why ASTP/ONC should advance the data element to enable standardized exchange across the various health care settings patients use. Otherwise, the ecosystem is left with fragmentation and significant potential for missing critical information and accommodation, duplicate testing, error, and adverse effects on patient safety and quality.
Mark Savage, Managing Director, Digital Health Strategy & Policy, Savage & Savage LLC
CDC supports CMS's comment for advancing Accommodation from Level 0 to Level 2, as it is essential for identifying and addressing patient-specific support needs, improving accessibility, and ensuring compliance with disability rights laws. This element enables more equitable, person-centered care across healthcare settings.
Recommendation: Advance the Accommodation (Level 0) data element to Level 2 in the Patient Demographics/Information data class within USCDI.
Rationale: CMS CCSQ supports advancing the Accommodation data element from Level 0 to Level 2. We recognize and appreciate inclusion of Accommodation at Level 0, which is an important first step toward increasing visibility into the barriers that individuals with disabilities and other needs face in healthcare settings.
Approximately 27% of U.S. adults live with some form of disability (CDC, 2023), many of whom experience significant health disparities, including limited access to providers and higher rates of chronic conditions. Additionally, an estimated 70 million Americans face challenges related to self-care, independent living, mobility, and cognition (CDC, 2024). These barriers are particularly prevalent among older adults and are often compounded by decreased social and community engagement, which contributes to secondary health conditions such as depression (CDC, 2024).
While the existing Disability Status element in USCDI identifies whether a patient has a disability, the Accommodation data element provides actionable detail about the specific modifications, supports, or technologies required to remove barriers to care and support daily living for those with accommodation needs that stem from a disability or some other reason. These include physical adjustments, communication supports, or policy modifications, allowing providers to tailor services to each patient’s unique needs. This reinforces the understanding that disability is not solely a health outcome, but a condition shaped by the interaction between a person and their environment—impacting hearing, vision, mobility, cognition, and self-care.
Documenting accommodation needs is also essential for ensuring compliance with legal requirements outlined in the Americans with Disabilities Act (ADA), Section 504 of the Rehabilitation Act, and Section 1557 of the Affordable Care Act, which require healthcare providers to offer reasonable accommodations. Inclusion of this data in EHRs enables proactive identification of needs, reduces the risk of noncompliance, and facilitates more inclusive, equitable care
The case for moving Accommodation from Level 0 to Level 2 is supported by several criteria for advancing elements in the USCDI:
Demonstrated Use:Accommodation data is already being collected and exchanged in several federal programs. Notably, the Post-Acute Care (PAC) Quality Reporting Programs (QRP) utilize the Functional Assessment Standardized Items (FASI) to gather standardized accommodation-related data (CMS, 2023). FASI includes the "Assistive Devices for Everyday Activities" section (Item ID GG0125), which captures the use of canes, crutches, walkers, communication devices, oxygen, ramps, and more (GG0125A–GG0125Z).
Standardization and Technical Maturity: Two important HL7 FHIR Implementation Guides (IGs), the PACIO Personal Functioning & Engagement (PFE) IG and the National Directory of Healthcare Providers and Services (NDH) IG, demonstrate that the data infrastructure needed for Accommodation is both defined and ready for integration into health IT systems.
The PACIO PFE IG defines a ValueSet focused on assistive products and technologies, which includes hearing aids (LOINC: 94900-8), communication devices (LOINC: 94901-6), wheelchairs, walkers, ramps, grab bars, vision aids, and other common supports. This IG, currently in trial use, provides a strong foundation for incorporating accommodations into patient records in a standardized format (HL7, PACIO PFE IG, 2024).
In parallel, the NDH IG includes an Accessibility ValueSet that defines accommodations offered by providers and facilities, including physical and communication supports such as accessible entrances, assistive listening devices, service animal policies, sign language interpretation, and accessible exam tables. Typically implemented through FHIR resources like Location, Organization, or Healthcare Service and currently in trial use, the IG allows provider directories and scheduling systems to expose availability of accommodations for patient matching and navigation (HL7, NDH IG, 2024).
Alignment with National Priorities: Capturing Accommodation data supports national priorities related to health equity, accessibility, and patient-centered care. The ASTP/ONC Health Information Technology Advisory Committee (HITAC) has explicitly recommended the inclusion of an Accommodation data element to USCDI, emphasizing its importance in delivering inclusive, responsive healthcare (HITAC, 2022).
Stakeholder and Policy Support: Providers, patients, advocacy groups, and federal entities have consistently emphasized the need to document and share accommodation needs across care settings. Routine documentation of accommodations supports compliance with disability rights laws, improves care coordination, and enhances person-centered care planning. It also enables longitudinal tracking of accommodation needs and functional status over time (Morris, 2024), aligning with federal recommendations for more inclusive health IT infrastructure
References:
Buning, G., James, T. E., Richards, B., & McKee, M. M. (2024). Self-reported accommodation needs for patients with disabilities in primary care. The Joint Commission Journal on Quality and Patient Safety, 49(12), 776–786. https://doi.org/10.1016/j.jcjq.2023.10.012
Morris, M. (2024). Documentation of disability status and accommodation needs in the electronic health record: A qualitative study of health care organizations’ current practices. The Joint Commission Journal on Quality and Patient Safety.
As members of the Strategic Team of the Hearing Loss Association of America’s Communication Access in Health Care program—and as individuals with profound hearing loss—we strongly support advancing the Accommodation data element from Level 0 to Level 2.
Failure to document the accommodations a patient requires to communicate effectively with their health care team jeopardizes the health and safety of the patient, compromises the provider’s ability to deliver the best care, and places the health care facility in an ethically and legally vulnerable position. Without proper documentation, the burden of ensuring effective communication falls unfairly on the patient.
Key barriers to communication access in medical facilities include:
A lack of awareness that more than 50 million Americans struggle to hear health information clearly.
Limited understanding among providers of the availability and benefits of appropriate aids and services.
The absence of systemic processes to ensure accommodations are implemented consistently.
We have personally experienced the physical and psychological ramifications that occur when we are unable to communicate with providers and staff, particularly in urgent situations. Through our advocacy work, we are also in contact with hundreds of others who share this tenuous position when seeking safe and equitable medical treatment.
Rationale for advancing the Accommodation data element:
Enables facilities to plan for the full range of accommodations patients may require.
Reduces barriers faced by patients with disabilities when their accommodation needs are not identified or met.
Supports compliance with legal mandates requiring reasonable accommodations.
Advancing the Accommodation data element is a critical first step toward removing these barriers and ensuring that all patients receive the safest, most equitable, and highest-quality care.
Toni Iacolucci & Peggy Ellertsen, Communication Access in Health Care program, Hearing Loss Association of America
Comments submitted by: Barbara Kelley, Executive Director, Hearing Loss Association of America
Accommodations are distinct from disability status and are critical for delivering person-centered care. Capturing this information in EHRs would:
Improve care coordination, especially during transitions between settings.
Reduce medical errors and enhance safety for individuals requiring specific supports.
Empower providers to meet legal and ethical obligations under the ADA and Section 504.
Hearing loss is a compelling example of why accommodations data is essential. For example,
More than 50 million Americans have some degree of hearing loss. That’s about 1 in 7 people in the U.S. (NIDCD and U.S. Census)
Hearing loss is the 3rd most common chronic physical condition in the U.S., twice as prevalent as diabetes or cancer. (CDC)
Hearing loss is associated with other common health issues such as diabetes and heart disease. (Healthy Hearing)
Hearing loss is on the rise and is expected to affect 2.5 billion people worldwide by 2050. (WHO)
12% of all U.S. workers report hearing difficulty. (CDC)
20% of noise-exposed workers have a material hearing loss that affects daily activities. (CDC)
13% of noise-exposed workers have hearing loss in both ears. (CDC)
These individuals may require accommodations such as assistive listening devices, captioning services, or communication support. Most people with hearing loss do not use sign language, so communication access beyond that is critical in a health care situation. Even a mild to moderate hearing loss can present barriers, especially hearing in noise. Without a standardized way to document these needs, care teams may miss critical information that affects communication, safety, and outcomes.
Recommendation:PACIO recommends advancement of the Accommodation data element from Level 0 to Level 2 in the Patient Demographics/Information data class.
Rationale: The PACIO Community* strongly supports the HITWG’s recommendation to advance the Accommodation data element from Level 0 to Level 2 in the Patient Demographics/Information data class. Accommodations are critical for ensuring that individuals with and without disabilities receive equitable, accessible, and patient-centered care. The Disability Status data element identifies the presence of a disability, which may be related to accommodation needs, the Accommodation data element provides actionable, individualized information about the specific support, modification, or technology needed to remove barriers to care and daily living. This includes physical adjustments, communication supports, and changes to a policy, practice or rule that should give a person equal access to facilities and services. Each accommodation enables providers to tailor services to each patient’s unique needs. Documenting the need for an accommodation is essential for compliance with federal laws such as the Americans with Disabilities Act (ADA), Section 504 of the Rehabilitation Act, and Section 1557 of the Affordable Care Act, all of which require healthcare providers to offer reasonable accommodations. Inclusion of this data element in EHRs facilitates proactive identification of needs, reduces risk of noncompliance, and supports more patient-centered care. Furthermore, advancing the Accommodation data element will address all needs identified in the Level 0 Communication Status data element, as the communication-based accommodation information is the primary means of supporting effective patient-provider interaction.
USCDI Level Criteria:
Current Standards: Level 2 – Accommodation data are represented by several terminology standards.
The PACIO Personal Functioning and Engagement (PFE) Implementation Guide (IG) STU2 defines a ValueSet focused on assistive products and technologies, leveraging standardized vocabularies such as LOINC and SNOMED CT. Examples include hearing aids (LOINC: 94900-8), communication devices (LOINC: 94901-6), wheelchairs, walkers, ramps, grab bars, vision aids, and other supports. These elements are designed for structured, computable capture in EHR systems, supporting interoperability and standardized exchange.
Current Use: Level 2 – Accommodation data are currently captured in multiple production EHRs from more than one developer.
Organizations capturing Accommodation include Epic and Cerner as documented in a recent Joint Commission journal article1. Another Joint Commission Journal article2 specifically noted that Epic enables the documentation of needed accommodation, including communication support, mobility aid, and cognitive support. The article highlights frequent requests for assistive listening devices, large-print materials, decision-making supports, and mobility assistance.
Current Exchange: Level Undetermined
Most organizations that currently collect this information use custom-built data collection within their EHRs or EMRs. The primary focus of this collection is to support patients’ needs during their associated healthcare visits. Currently, there is no evidence to suggest that this information is being exchanged.
Breadth of Applicability: Level 2 – Use cases for Accommodation data apply to most care settings.
Accommodation data are collected and used across a wide range of healthcare settings, as indicated in the Joint Commission journal article1 that reported on Accommodation information being collected across various hospitals and clinics.
Additional Note: The PACIO Community will end recommendations for the advancement of the Communication Status data element (Level 0) in favor of advancing the Accommodation data element, as the latter fully addresses the needs identified in the Communication Status data element, particularly the ability to record and exchange information about communication-based supports and technologies.
References:
Morris, M. A., Sarmiento, C., & Eberle, K. (2024). Documentation of disability status and accommodation needs in the electronic health record: A qualitative study of health care organizations’ current practices. The Joint Commission Journal on Quality and Patient Safety, 50(1), 16–23. https://doi.org/10.1016/j.jcjq.2023.10.006
Buning, G. E., James, T. G., Richards, B., & McKee, M. M. (2024). Self-reported accommodation needs for patients with disabilities in primary care. The Joint Commission Journal on Quality and Patient Safety, 50(1), 59–65. https://doi.org/10.1016/j.jcjq.2023.10.012
* The PACIO (Post-Acute Care Interoperability) Project, established February 2019, is a collaborative effort between industry, government, and other stakeholders, that aims to advance interoperable health information exchange between post-acute care (PAC) providers, patients, and other key stakeholders across health care.
The "Optional Background Text / Cover Letter" field provides space for additional context or introductory information related to your comment.
If you wish to provide context, explanation, or an introduction to your comment, enter this information in the field labeled "Optional Background Text / Cover Letter." This is entirely optional and is most useful when submitting multiple related comments or when additional background would help reviewers understand your feedback.
If you are only commenting on a single data class or element, you may leave this field blank.
2. Select the Data Class
To specify which data class your comment addresses:
In the "Data Class" drop-down menu, select the appropriate data class you want to comment on.
If you are providing a general comment that is not specific to a data element, select "General" from the options. Comments with this designation will be displayed on the USCDI landing page.
Note that the Data Class field will automatically populate based on your current location in the platform:
If you are on a data class page, the field will be set to that specific data class
If you are on a data element page, the corresponding data class will be pre-selected
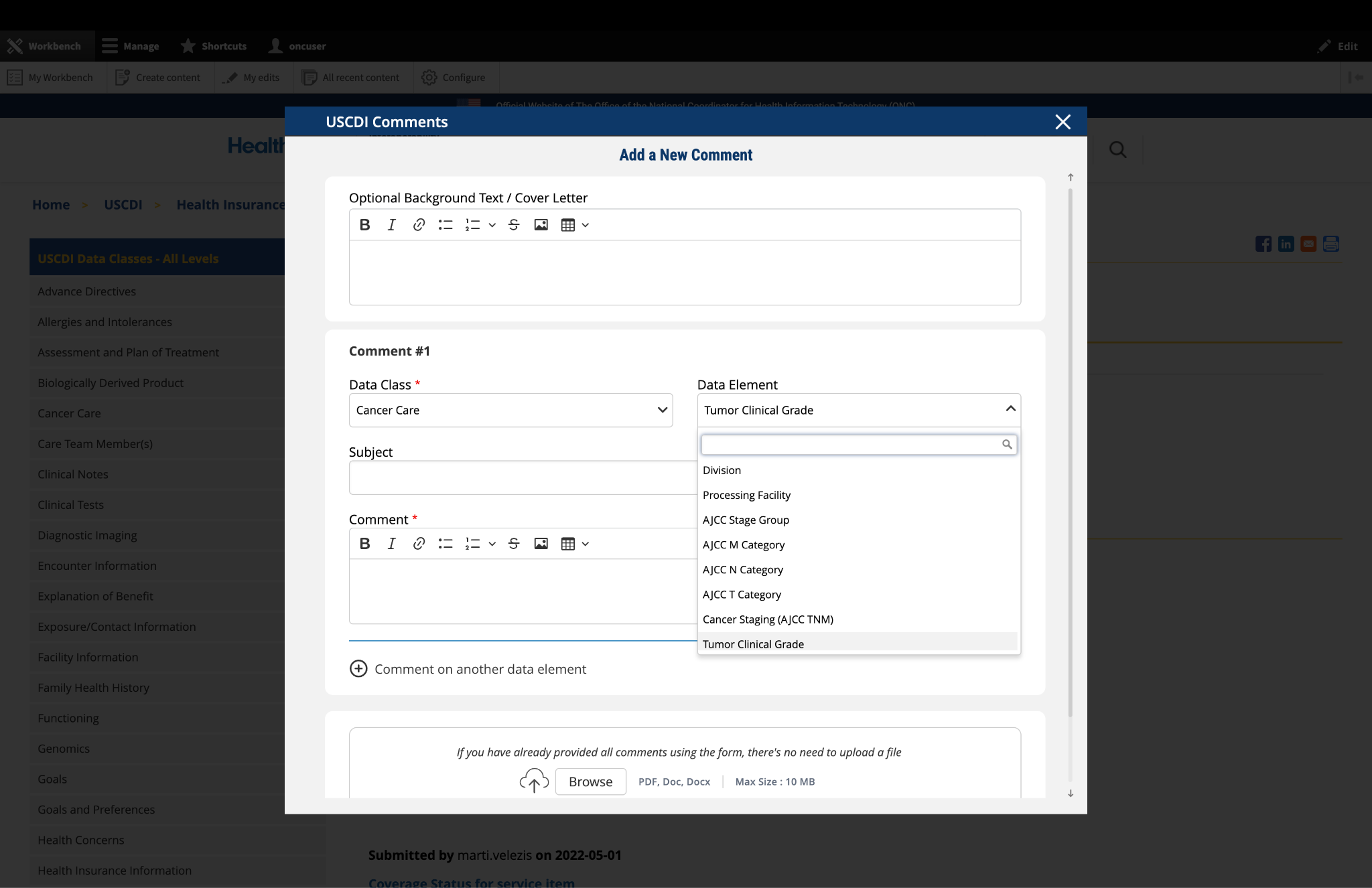
3. Select the Data Element
To specify which data element your comment addresses:
In the "Data Element" drop-down menu, select the specific data element you want to comment on.
The drop-down menu will display only the elements available under the data class you selected in the previous step.
You can use the search function within the drop-down to quickly locate a specific data element.
If you are commenting on the data class itself rather than a specific element, you may leave this field blank.
Note: Comments on a specific data element will appear on the respective data element page, while comments on a data class (without a specific element selected) will appear on the landing page for that data class.
Fig 1 The "Data Class" and "Data Element" dropdown menus allow users to specify the exact content they wish to comment on.
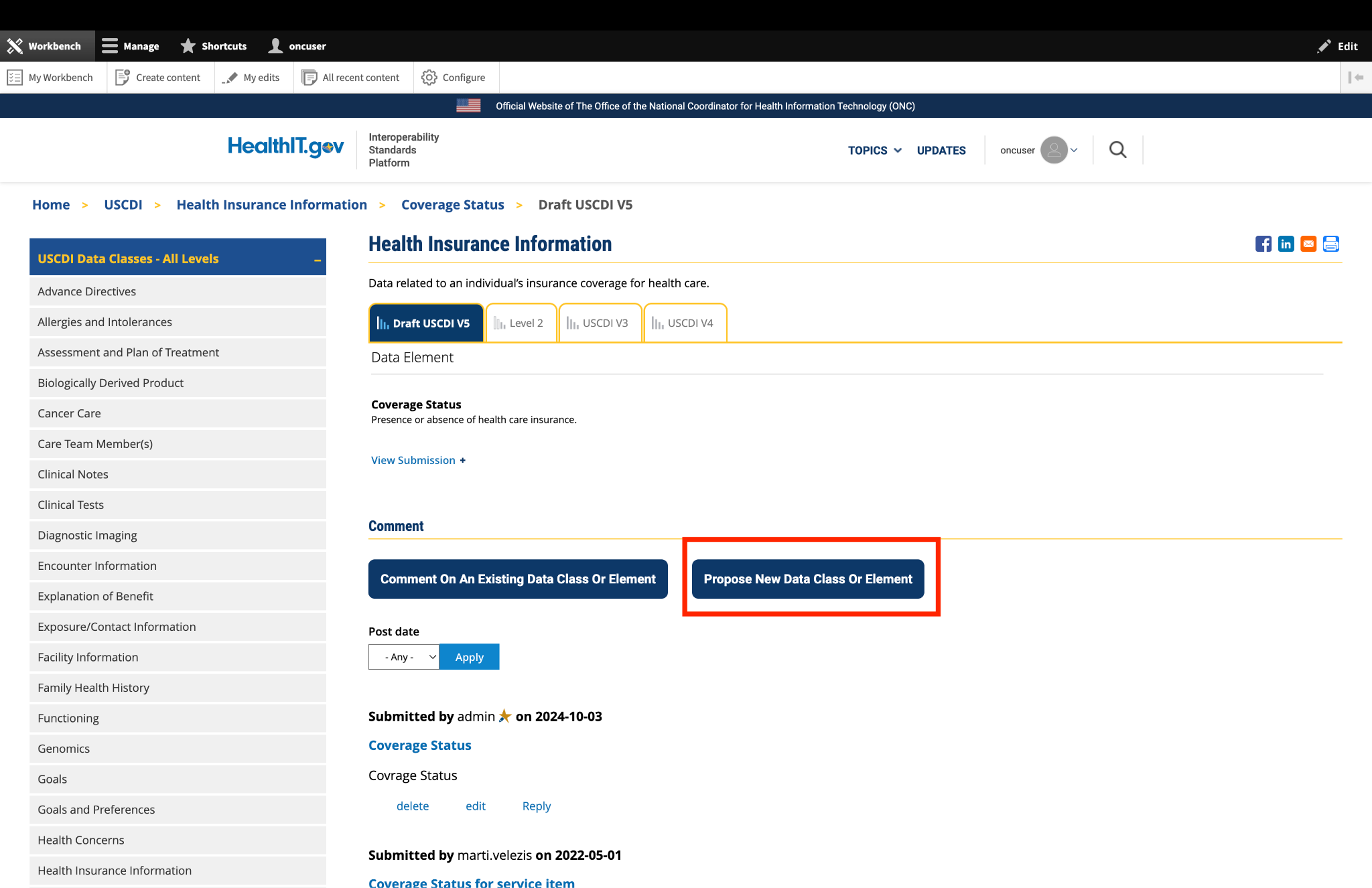
4. Optional: Propose New Data Class or Element
If you cannot find the appropriate data class or element for your comment:
Instead of clicking the "Comment On An Existing Data Class Or Element" button, click the adjacent button labeled "Propose a New Data Class or Data Element."
This will redirect you to the ONDEC (ONC New Data Element and Class) Submission System.
In the ONDEC system, follow the provided instructions to submit your proposal for a new data class or element.
Once your proposal is submitted through ONDEC, it will be reviewed separately from the commenting process.
Fig 2 The "Propose a New Data Class or Data Element" button redirects users to the ONDEC Submission System for proposing new data elements not currently available in the system.
5. Complete the Comment Form
Fill out the required fields in the comment form:
Subject: Enter a brief, descriptive title that summarizes your comment. This helps reviewers quickly understand the nature of your feedback.
Comment: In this field, provide the full details of your comment or feedback. Be as clear and specific as possible about your suggestions, concerns, or observations. Include any relevant details that support your position.
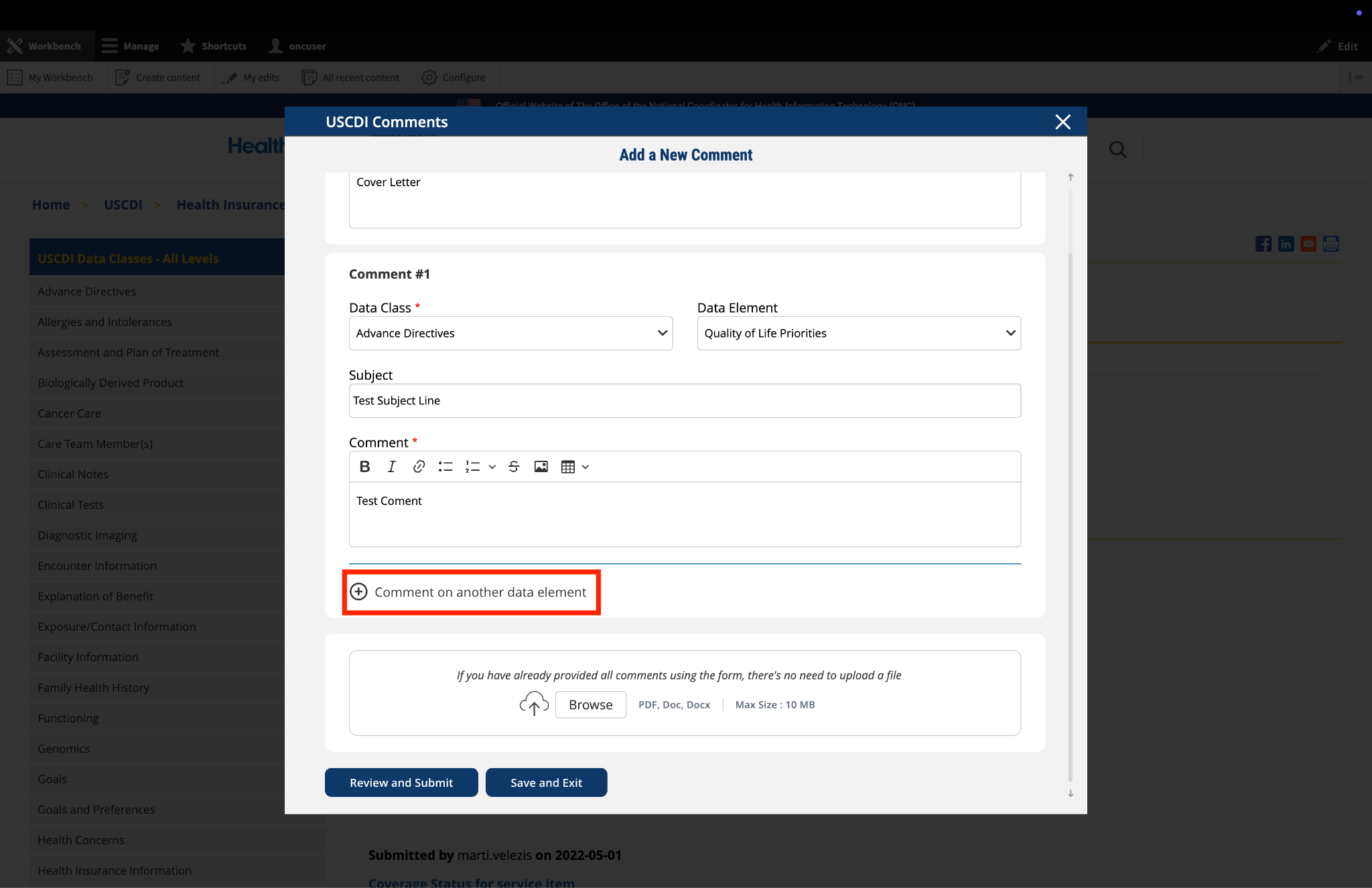
6. Optional: Add Additional Comments
If you need to comment on multiple data classes or elements:
After completing your first comment, click the link labeled "Comment on another data element" at the bottom of the form.
A new comment section will appear, allowing you to enter details for your additional comment.
For each additional comment, you must select the appropriate data class and data element from the drop-down menus.
Complete the Subject and Comment fields for your additional comment.
Repeat this process for each additional comment you wish to submit.
Fig 3 The "Comment on another data element" link enables users to create multiple comments addressing different elements within a single submission.
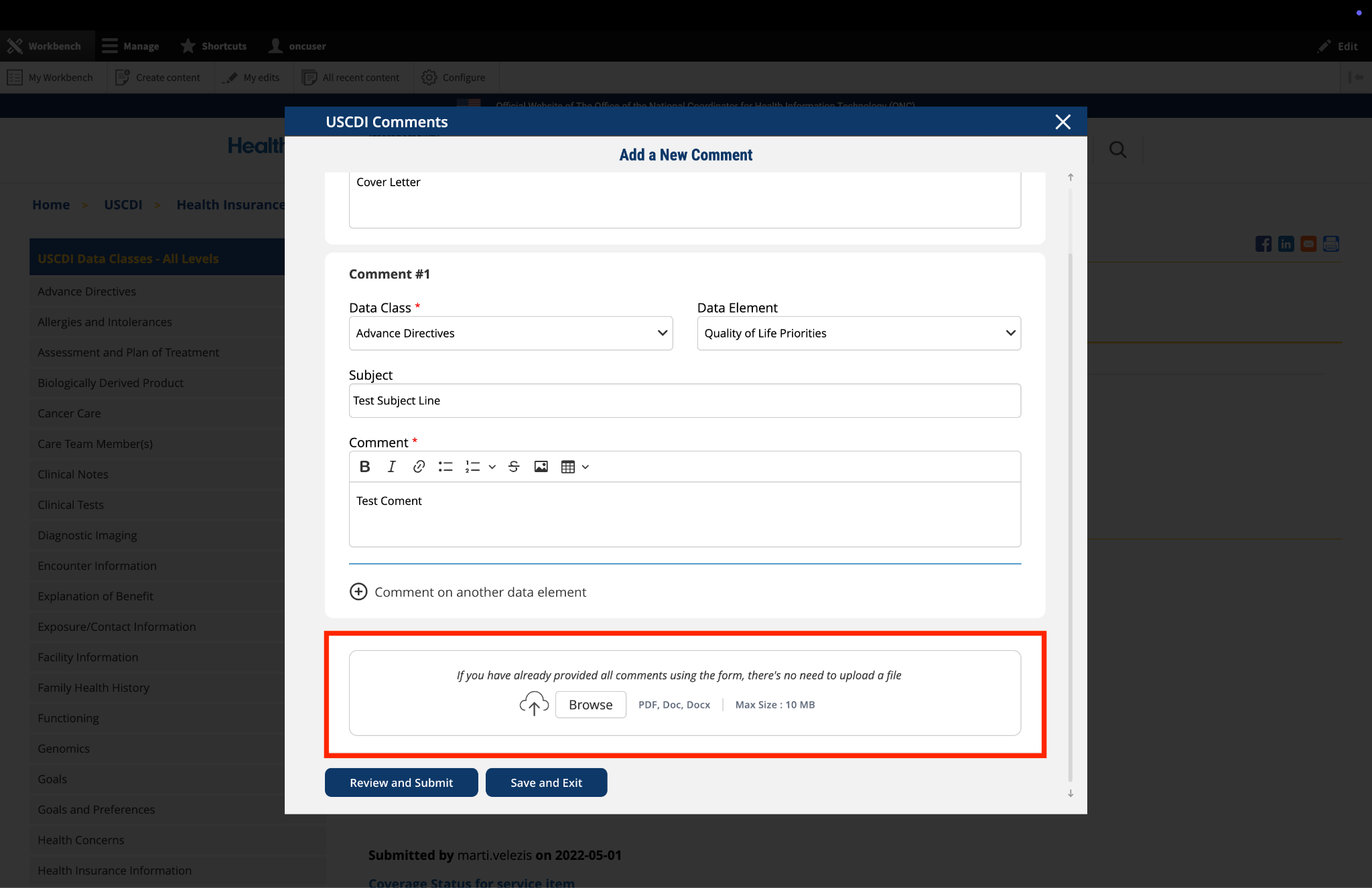
7. Optional: Upload Supporting Files
The platform allows you to upload supporting documentation to enhance your comment:
Locate the "File Upload" section at the bottom of the comment form.
Click to upload any files (such as PDFs or documents) that provide additional context, evidence, or clarification for your comment.
Important: If you have already entered your comments using the form fields, there is no need to upload duplicate content in PDF format. The file upload feature is intended for supplementary materials only. Please avoid uploading files that contain the same information already provided in your comment text.
Fig 4 The "File Upload" section permits users to attach supporting documentation that supplements their written comments.
8. Optional: Save and Exit
If you need to pause your work and return to complete your comment later:
Click the "Save and Exit" button at the bottom of the form.
Your comment will be saved as a draft that you can access and complete later.
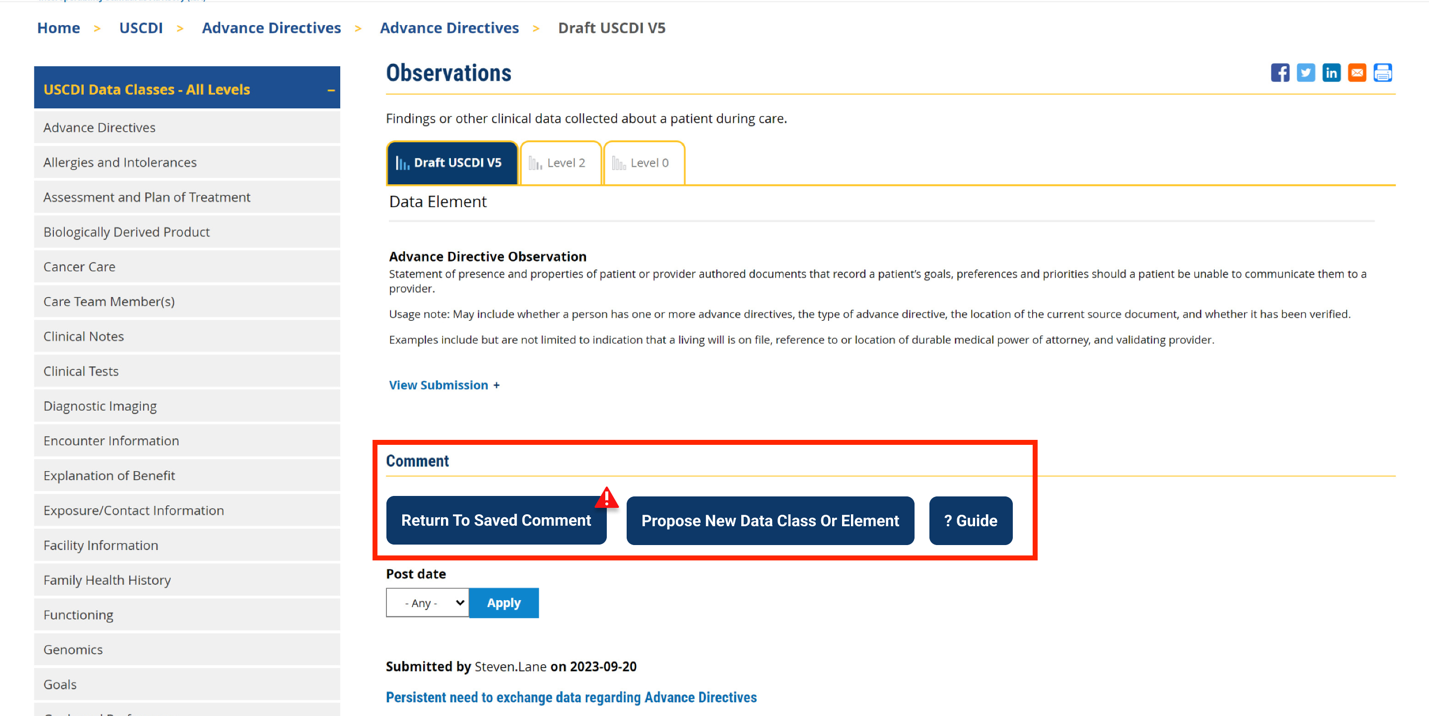
When you return to the platform, you will see a red triangle with an exclamation mark next to the “Return to saved Comment” button, indicating that you have saved comments in draft status.
Click this button to continue working on your draft.
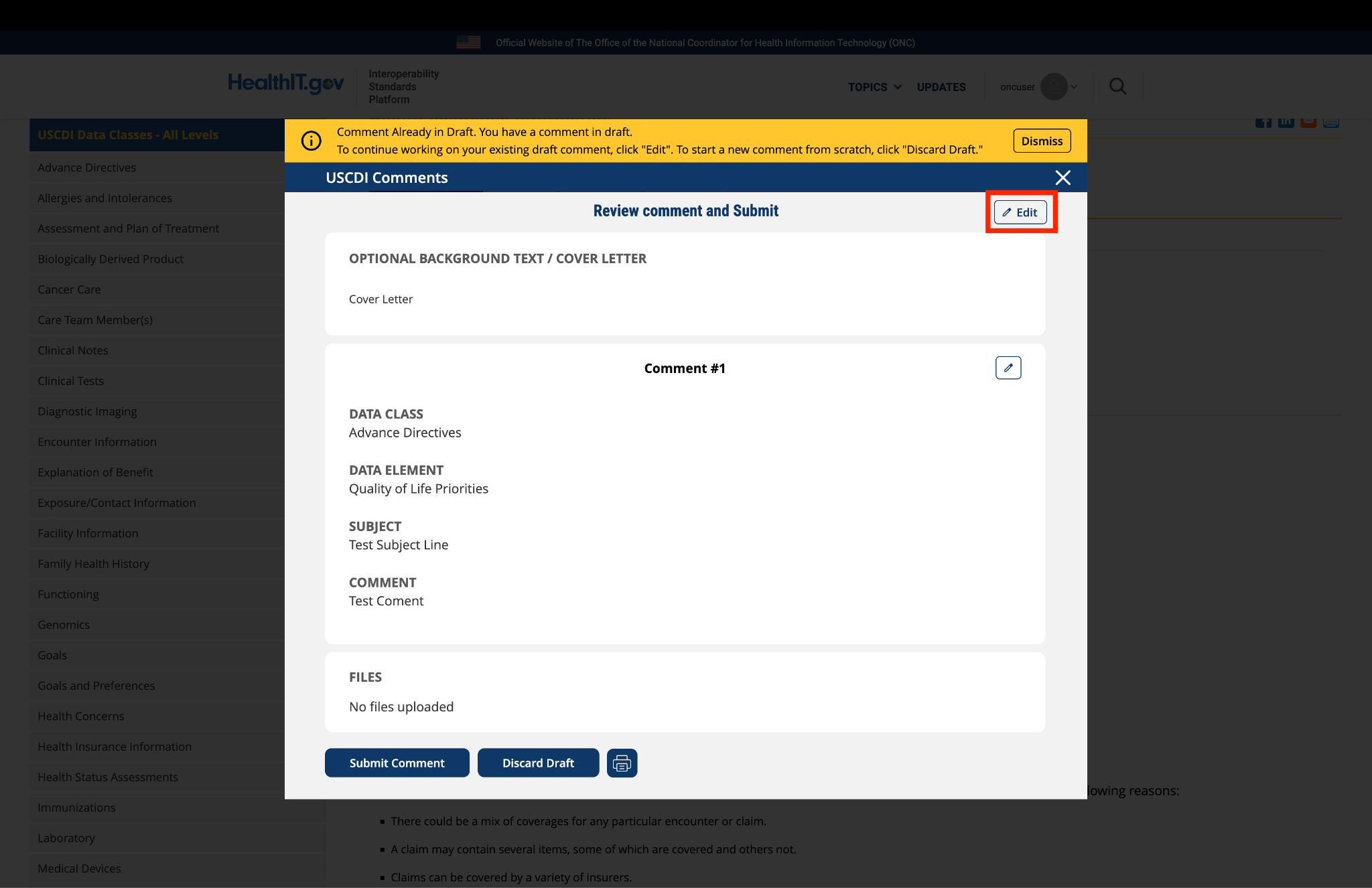
You will be taken to a review page where you can:
Select "Submit Comment" to officially submit your feedback.
Click "Edit" to return to the comment form and make changes
Select "Discard Draft" to delete the saved draft and start fresh
Fig 5 A red triangle with exclamation mark indicator appears next to the “Return to saved Comment” button when draft comments are saved in the system.
9. Review and Submit
Once you have completed your comment:
Click the "Review and Submit" button at the bottom of the form.
This will take you to a review screen displaying your comment(s) in full.
Review all information for accuracy and completeness.
On this review screen, you have three options:
Click "Submit Comment" to officially submit your feedback
Click "Edit" to return to the comment form and make changes
Click "Discard Draft" to delete the comment and start fresh
The review screen also includes a "Print" button that allows you to create a printed copy of your comments for your records.
If you choose to submit, your comment will be recorded in the system and made available for review by the appropriate stakeholders.
Fig 6 The review screen allows users to verify comment content and make any necessary modifications before final submission.


Submitted by rdillaire on
CMS-CCSQ Applauds this data element’s inclusion in USCDIv7
CMS CCSQ supports the inclusion of Accommodation in USCDI v7.