
Submitted by rdillaire on
CMS-CCSQ Applauds this data element’s inclusion in USCDIv7
CMS CCSQ supports the inclusion of Allergy Intolerance Criticality in USCDI v7.
 Official Website of the Office of the National Coordinator for Health Information Technology
Official Website of the Office of the National Coordinator for Health Information Technology
Harmful or undesired physiological responses associated with exposure to a substance.
Data Element |
||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Allergy Intolerance Criticality
Description (*Please confirm or update this field for the new USCDI version*)
Estimate of the potential clinical harm, or seriousness, of a reaction to an identified substance. | ||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||
Submitted by rdillaire on
CMS CCSQ supports the inclusion of Allergy Intolerance Criticality in USCDI v7.
Submitted by AmyJDalmas on
The proposed Criticality data element has the following note for implementation challenges: “Educational awareness for clinicians will be necessary since this field has replaced severity in clinical practice.” We request that this statement be rephrased, as this element has not replaced severity in clinical practice. Severity is the clinical assessment of a specific allergic reaction when it occurs (e.g., mild, moderate, severe). Criticality is an estimate of the potential clinical harm, or seriousness, of a reaction to an identified substance (e.g., low, high, unknown). Clinicians use both severity and criticality in practice to diagnose and treat allergies and intolerances. In some systems, criticality may be derived, in part, by the severity of a previous reaction. We propose changing the Criticality data element note to the following: “Educational awareness for clinicians may be necessary since this field can be derived from severity or has replaced severity in some clinical systems.” Also, there is a Level 2 USCDI element Reaction Severity that we support being added to future versions of the USCDI data standard.
Submitted by AAAAI on
The American Academy of Allergy, Asthma & Immunology (AAAAI) strongly supports the proposed addition of Allergy Intolerance Criticality as a data element within the United States Core Data for Interoperability (USCDI). The AAAAI represents thousands of allergist-immunologists dedicated to improving the diagnosis, treatment and documentation of allergic and immunologic diseases. We believe this proposed change directly advances patient safety, enables better clinical decisions, and lays critical groundwork for the broader modernization of allergy documentation in electronic health records (EHRs).
Why the AAAAI Supports This Change
The current allergy module in most EHRs fails to adequately communicate the clinical criticality of documented reactions. At present, a patient with a history of anaphylaxis to penicillin and a patient with a mild gastrointestinal intolerance to the same drug often carry identical allergy labels, an ambiguity that impairs clinical decision-making and contributes to unnecessary drug avoidance. The proposed Allergy intolerance Criticality data element, offering standardized coded values of Low Criticality, High Criticality, and Unable to Assess, addresses this gap directly. Its addition is crucial to improve patient safety and will result in better outcomes by not avoiding drugs with low risk in favor of treating a disease with high risk of morbidity. By enabling clinicians to distinguish potentially life-threatening reactions from less severe ones, this element supports more actionable, proportionate clinical responses across care settings.
However, although the Standards Bulletin announcing version 7 of USCDI shows the Criticality data element is included, it does not have a bold S next to it. This means that it is suggested as “should support”. We strongly recommend that this important data element should be designated as Must Support.
Critically, standardizing this data element through USCDI will promote consistent implementation across EHR vendors, reduce reliance on free-text entries, and enable clinical decision support tools to better prioritize allergy alerts. This has the potential to meaningfully reduce alert fatigue—a well-documented problem that leads clinicians to override warnings that may, in some cases, represent true safety hazards.
Context: AAAAI’s Ongoing Work on EHR Allergy Documentation
The AAAAI has been a leading voice in advocating for the modernization of allergy documentation within electronic health records. We are eager to collaborate with the ONC, EHR vendors, and other healthcare stakeholders to implement standardized frameworks that move beyond the limitations of current systems, such as over-reliance on free-text and inconsistent terminology. While the addition of Allergy Intolerance Criticality is a meaningful and necessary first step, we remain enthusiastic about sharing our broader vision for more precise, actionable documentation, including improved hierarchical categorization and enhanced clinical decision support, to ensure patient safety and reduce clinician alert fatigue across all care settings.
The USCDI as Foundation for Future Progress
The AAAAI views the USCDI standards as foundational infrastructure upon which future progress in allergy documentation must be built. Standardized, coded data elements, exchanged interoperably across systems, are a prerequisite for the more advanced reforms our field envisions: improved allergy delabeling workflows, natural language processing–assisted reconciliation, genetic and pharmacogenomic risk integration, and cross-institutional alert exchange that does not depend solely on patient self-report. Without alignment at the USCDI level, locally implemented improvements will remain siloed and unable to achieve population-level safety gains.
The AAAAI is committed to serving as a resource to ONC, EHR vendors, and other stakeholders as this work continues. We encourage ONC to finalize the inclusion of Allergy Intolerance Criticality in the USCDI, but to change its designation to Must Support.
Respectfully submitted,
Carla M. Davis, MD, FAAAAI
President, American Academy of Allergy, Asthma & Immunology
Submitted by SuzyRoy on
SNOMED International recommends that ONC designate SNOMED CT U.S. Edition as an applicable vocabulary standard for Allergy Intolerance Criticality.
SNOMED CT includes validated clinical severity and risk concepts, such as 24484000 |Severe (severity modifier)|, 6736007 |Moderate (severity modifier)|, and 255604002 |Mild (qualifier value)|. This provides a clinically precise vocabulary for criticality assessment, enabling consistent risk stratification across EHR and clinical decision support systems. Designating SNOMED CT for this element ensures intra-class consistency: SNOMED CT is already required for Drug Class Allergy Intolerance, Non-Medication Allergy Intolerance, and Reaction within the same Allergies and Intolerances data class.
Allergy Intolerance Criticality is a patient safety data element with direct clinical decision support implications. Inconsistent coding of criticality severity across systems creates risk of medication errors and inappropriate care decisions, particularly in emergency and cross-organisational settings where allergy data must be reliably exchanged. SNOMED CT designation as the applicable standard for this element supports ONC's Clinical Decision Support (CDS) certification criteria, which reference SNOMED CT as a core clinical terminology for condition and severity coding, and aligns with the patient safety objectives of the 21st Century Cures Act's information blocking provisions.
Submitted by jay.lyle@jpsys.com on
Criticality evidence would be more useful than judgment
The criticality requirement envisions a scenario where the documenting provider has information about criticality that the receiving provider does not have. It would be good for the receiving provider to have this information.
But it's not clear that asking prior providers to assign criticality judgments will bring this about. Criticality judgments without evidence add burden to the recording provider, potentially degrading data quality, without a clear benefit to the receiver.
Criticality judgments can often be inferred based on known combinations of medication & symptom, such as 'penicillin + dyspnea' or 'morphine + nausea'. Adding such a judgment provides little value to the receiver.
A criticality judgment might provide value if it deviates from clinical norms, but without supporting evidence it might only create ambiguity. In a high-acuity setting, a 'High' criticality rating for a common, non-severe reaction (like nausea) without evidence why the provider determines that this case is different could lead to unnecessary care delays or diagnostic distraction.
Criticality evidence (optional) would be useful in such cases.
If we wish to support less knowledgeable providers by (possibly automatically) assigning judgment based only on clinical norms, this assignment should also be explicit about the rationale for the assignment (e.g., "expected criticality for this substance & reaction pair; no additional information".
Submitted by CDC_DSMH_WG on
CDC supports CMS recommendation for adding Criticality to final USCDI v7
Submitted by rdillaire on
Recommendation: CMS CCSQ recommends the Criticality element be added to final USCDI v7.
Rationale: CMS CCSQ supports Post-Acute Care Interoperability (PACIO)’s recommendation to include the Criticality data element in USCDI v7. Adding this data element to the Allergies and Intolerances data class is essential for improving patient safety and clinical decision-making. The Criticality data element complements existing USCDI elements by providing critical, clinically actionable information about the severity and potential impact of allergic reactions, enabling healthcare providers to better assess risks and prioritize care. Under the administration’s priorities, CMS CCSQ and PACIO share a commitment to improving national prevention of poor health through the avoidance of allergic reactions experienced under the care of health providers by enhancing data exchange and empowering providers to make informed, patient-centered decisions.
Submitted by jpatterson@mitre.org on
Submitted by rdillaire on
Recommendation: CMS CCSQ recommends the Criticality element be added to final USCDI v6.
Rationale: CMS CCSQ supports Post-Acute Care Interoperability (PACIO)’s recommendation to include the Criticality data element in USCDI v6. Adding this data element to the Allergies and Intolerances data class is essential for improving patient safety and clinical decision-making. The Criticality data element complements existing USCDI elements by providing critical information about the severity and potential impact of allergic reactions, enabling healthcare providers to better assess risks and prioritize care. CMS CCSQ and PACIO share a commitment to enhancing data exchange and empowering providers to make informed, patient-centered decisions.
The "Optional Background Text / Cover Letter" field provides space for additional context or introductory information related to your comment.
If you wish to provide context, explanation, or an introduction to your comment, enter this information in the field labeled "Optional Background Text / Cover Letter." This is entirely optional and is most useful when submitting multiple related comments or when additional background would help reviewers understand your feedback.
If you are only commenting on a single data class or element, you may leave this field blank.
To specify which data class your comment addresses:
To specify which data element your comment addresses:
Note: Comments on a specific data element will appear on the respective data element page, while comments on a data class (without a specific element selected) will appear on the landing page for that data class.
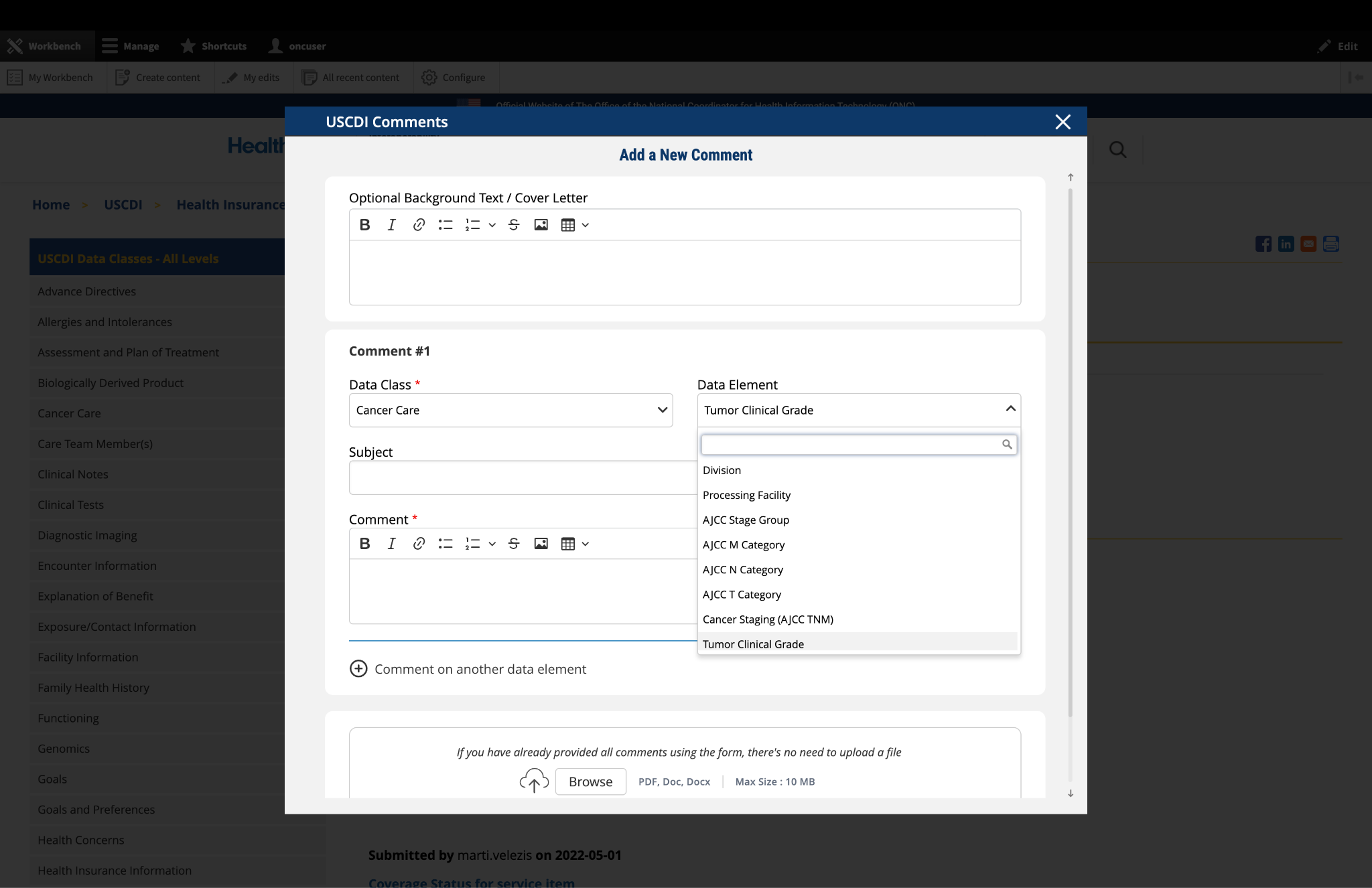
Fig 1 The "Data Class" and "Data Element" dropdown menus allow users to specify the exact content they wish to comment on.
If you cannot find the appropriate data class or element for your comment:
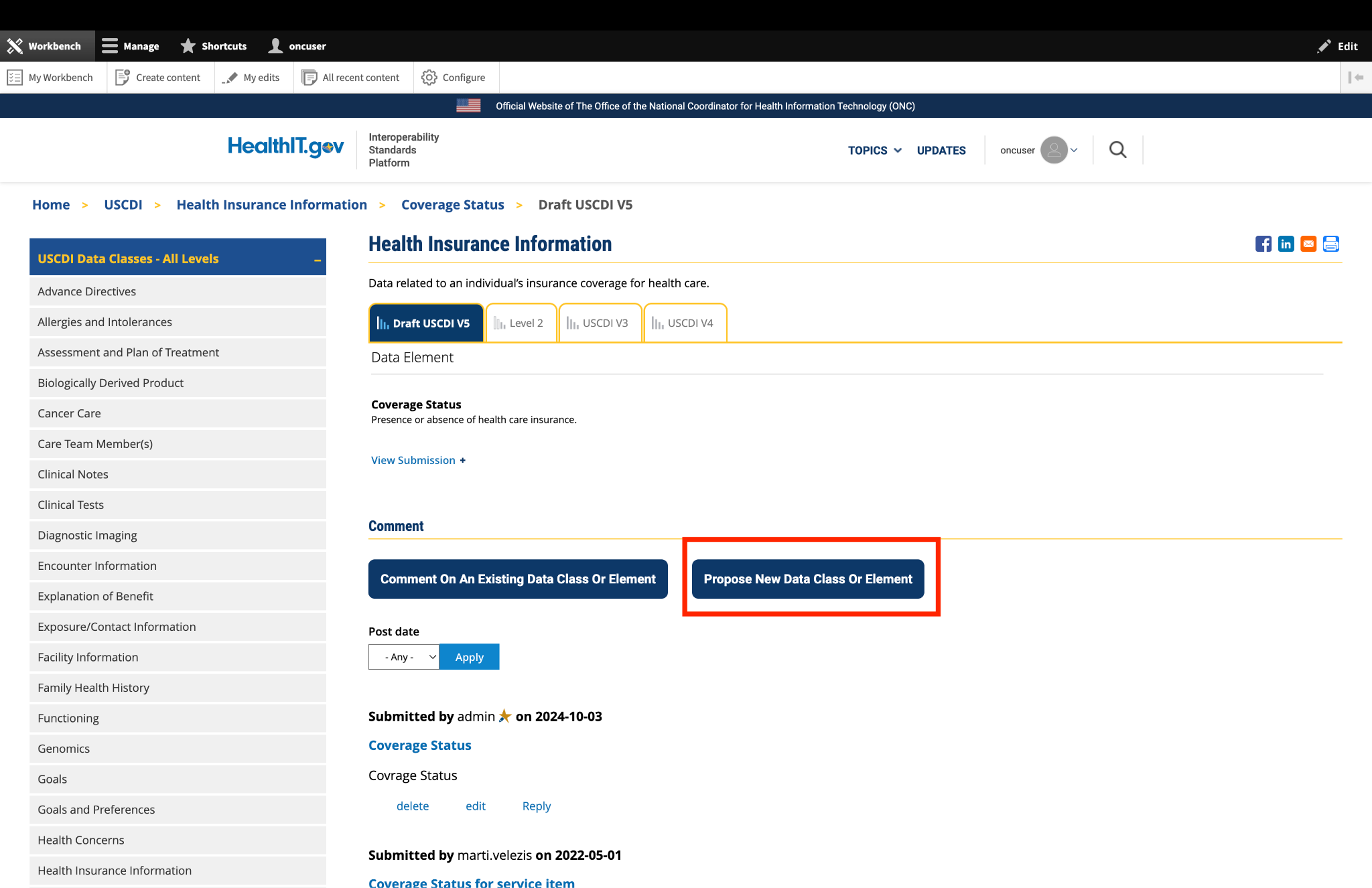
Fig 2 The "Propose a New Data Class or Data Element" button redirects users to the ONDEC Submission System for proposing new data elements not currently available in the system.
Fill out the required fields in the comment form:
Subject: Enter a brief, descriptive title that summarizes your comment. This helps reviewers quickly understand the nature of your feedback.
Comment: In this field, provide the full details of your comment or feedback. Be as clear and specific as possible about your suggestions, concerns, or observations. Include any relevant details that support your position.
If you need to comment on multiple data classes or elements:
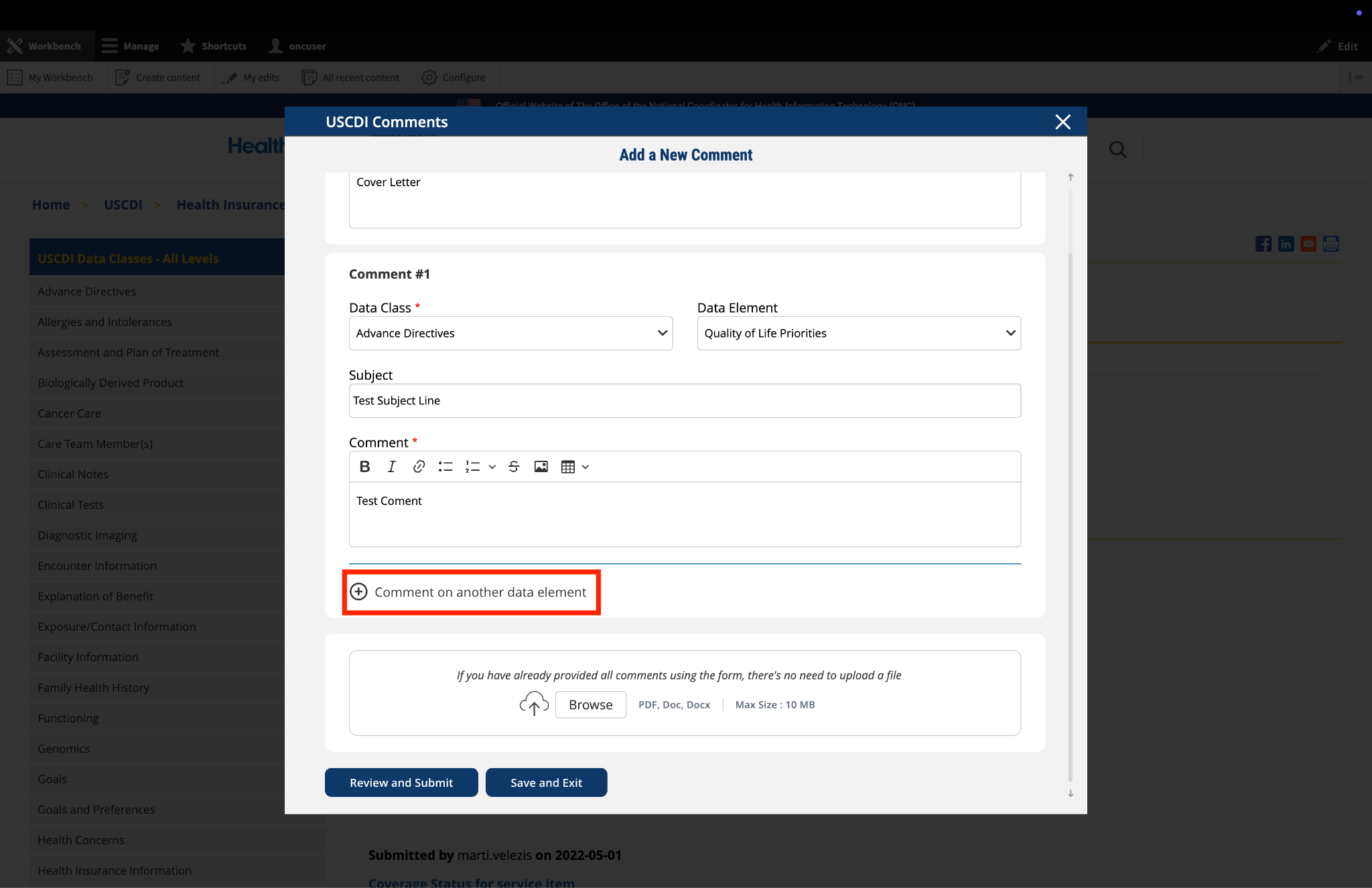
Fig 3 The "Comment on another data element" link enables users to create multiple comments addressing different elements within a single submission.
The platform allows you to upload supporting documentation to enhance your comment:
Important: If you have already entered your comments using the form fields, there is no need to upload duplicate content in PDF format. The file upload feature is intended for supplementary materials only. Please avoid uploading files that contain the same information already provided in your comment text.
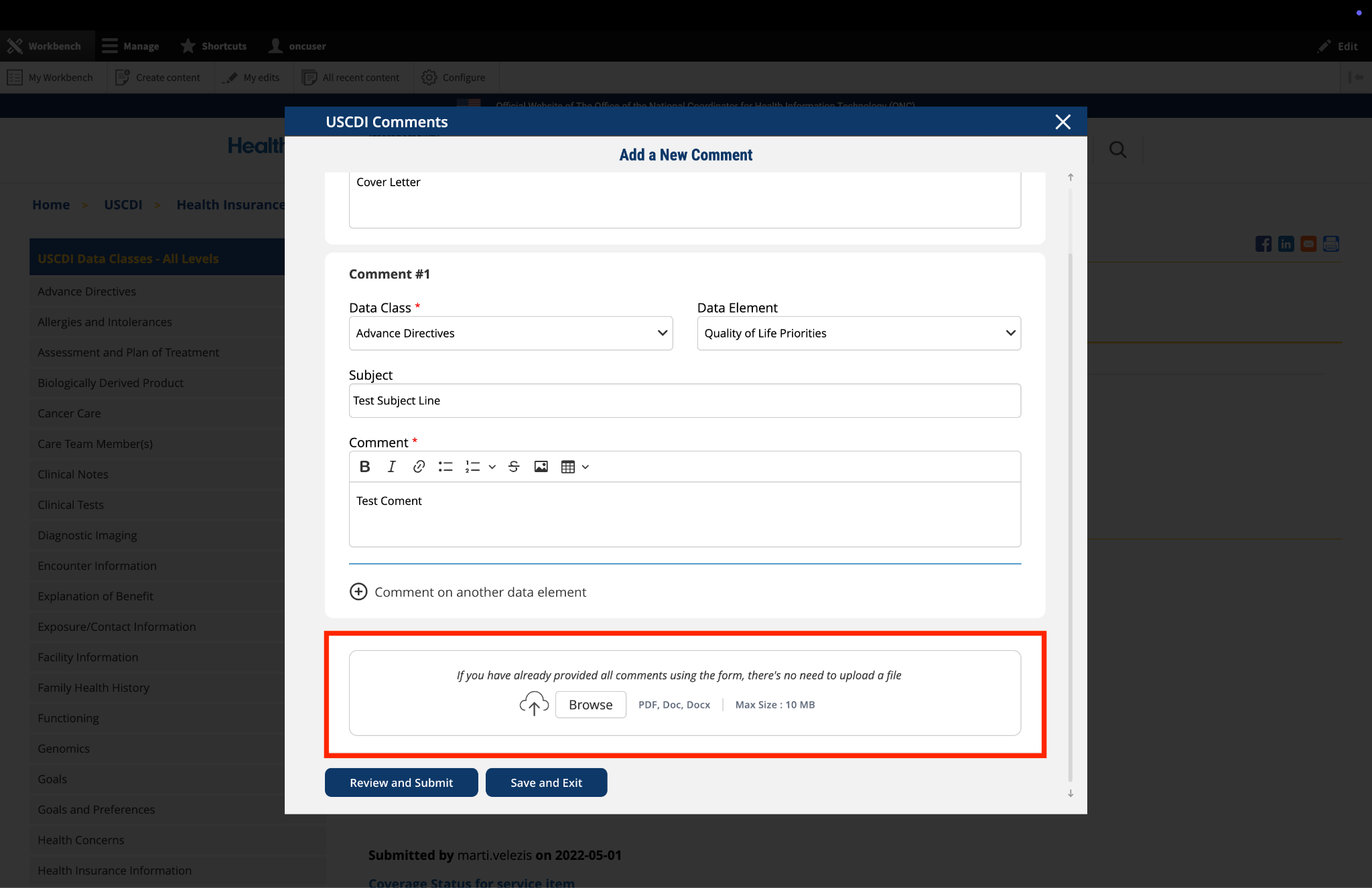
Fig 4 The "File Upload" section permits users to attach supporting documentation that supplements their written comments.
If you need to pause your work and return to complete your comment later:
Fig 5 A red triangle with exclamation mark indicator appears next to the “Return to saved Comment” button when draft comments are saved in the system.
Once you have completed your comment:
Fig 6 The review screen allows users to verify comment content and make any necessary modifications before final submission.
Submitted by EmoryHealthcare on
Emory Healthcare comments on Criticality
EHC strongly supports the proposed addition of Allergy Intolerance Criticality as a data element within the United States Core Data for Interoperability (USCDI). However, we also recommend further differentiation within the 'Allergy and Intolerance' section, which currently aggregates allergic reactions, non-allergic adverse drug reactions, side effects, and intolerances. We recommend segmenting drug reactions from the following classifications:
Drug Allergies: We see a clear and significant use case for criticality in specific scenarios, particularly with drug allergies where cross-reactivity and severe systemic reactions are well-documented. A standardized criticality here is invaluable for immediate patient safety.
Foods and Other Agents: For food allergies, environmental allergies, or other agents that may have less significant cross-reactivity or direct disease-food interactions, the utility of a "criticality" classification can be less pronounced. The clinical impact often varies widely, and a blanket application might not always be beneficial.
We also note that Provenance of these data is vital, as what patients might perceive as severe discomfort or significant impact on their quality of life might not necessarily equate to a high-risk medical event. This inherent subjectivity makes it difficult to consistently apply a standardized criticality. Despite these challenges, we strongly agree with the need for a national standard to classify criticality. A simplified, standardized approach, such as classifying criticality into low, high, and unable to assess risk, would greatly simplify the classification process and improve consistency across systems. This approach could provide actionable information while acknowledging the complexities of certain reactions and data input. We recommend that the ONC continue to emphasize and potentially further define the requirements for capturing and exchanging Allergy and Intolerance Criticality, while also providing clear guidance on its appropriate application and the need for a simplified, nationally standardized classification system (e.g., low, high, unable to assess risk).
2026 Emory Healthcare USCDI_v7 Comment Letter.pdf