Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Description (*Please confirm or update this field for the new USCDI version*)
State or condition of being pregnant or intent to become pregnant.
Examples include but are not limited to pregnant, not pregnant, and unknown.
Submitted By: Adam Bazer, MPD
/ Integrating the Healthcare Enterprise USA (IHE USA)
Data Element Information
Data Element Description
Pregnant, not pregnant, possibly pregnant
Use Case Description(s)
Use Case Description
A 24 year old female is being transported to a hospital for abdominal pains. During her transport she indicated that she is several weeks pregnant so the transport team makes sure to bring her to a hospital that has OBGYN capability. When she is in the hospital that pregnancy status indicator helps inform the providers to do some tests to make sure this pain is not related to her pregnancy and to avoid procedures that may have negative effects on the fetus.
Estimate the breadth of applicability of the use case(s) for this data element
This indication of pregnancy can be important for a variety of health care providers to help make informed decisions for the care of a patient. This would be captured and used in by any provider that creates or utilizes a patient electronic health record. This also may be populated by the patient in a personal record or at an appointment.
This data element has been used at scale between multiple different production environments to support the majority of anticipated stakeholders
Supporting Artifacts
HL7 FHIR Connecathon has trested the FHIR Pregnancy Status for eCR and the International Patient Summary in September 2020
Extent of exchange
5 or more. This data element has been tested at scale between multiple different production environments to support the majority of anticipated stakeholders.
Supporting Artifacts
HL7 FHIR Connecathon has trested the FHIR Pregnancy Status for eCR and the International Patient Summary in September 2020
Potential Challenges
Restrictions on Standardization (e.g. proprietary code)
none
Restrictions on Use (e.g. licensing, user fees)
none
Privacy and Security Concerns
none
Estimate of Overall Burden
This is regularly tracked as part of electronic medical records
CSTE continues to support pregnancy status as included data element in USCDI v7. However, a single variable is not sufficient to capture critical data that are needed for a large variety of conditions affecting the public's health, including maternal mortality, Hepatitis B and C, COVID-19, Zika, syphilis, and influenza, to name only a few. Additionally, the element description, which includes intent to become pregnant, should be revised to be simply 'current pregnancy status' - indicating whether the person is pregnant, not pregnant, or unknown. See CSTE's previous comments on pregnancy-related data elements.
I concur with Lisa Nelson's statement on Pregnancy Status that was commented on USCDI+ for maternal health for Pregnancy Status.
"Pregnancy status data element is a primary driver of the collection of Pregnancy Information. This is a well-established data element already carried in C-CDA R3.0 and should be included in the USCDI Level-0 Pregnancy Information Data Class."
Health Status – Pregnancy Status and Pregnancy Episode | Women’s Health
Maternal morbidity and mortality remain significant public health concerns in the United States, particularly among medically underserved and uninsured populations that community health centers serve. Standardizing critical pregnancy-related data in electronic health records (EHRs) is crucial for informing care decisions, coordinating maternal care, and improving care quality.
The CDC's Division of Reproductive Health, in collaboration with the National Association of Community Health Centers (NACHC), has made substantial progress in enhancing the quality of pregnancy and postpartum care within Federally Qualified Health Centers (FQHCs). By leveraging Health Information Technology (HIT) systems, they have successfully tracked and analyzed pregnancies, identified high-risk cases, and improved data standardization in EHRs. The initiative has revealed significant gaps in maternal care quality in community health centers.
The inclusion of standardized data elements like Pregnancy Status, Estimated Date of Delivery, and Pregnancy Outcome in the U.S. Core Data for Interoperability (USCDI) is crucial for improving maternal healthcare, research, and quality measurement. This is especially important for conditions like hypertensive disorders of pregnancy, which disproportionately affect certain demographics, including Black and Native American/American Indian individuals. NACHC has worked with multiple national health center-controlled networks to implement and extend the pregnancy episode as a longitudinal concept in multiple certified health IT products and therefore should we believe be considered at full maturity in Level 2.
Pregnancy Episode was previously proposed and submitted by NACHC in coordination for consideration to ONC since 2022. While NACHC agrees that there is a critical need for the pregnancy status data element, the currently submitted concept profile We recommend updating the submission which does not harmonize with electronic case reporting (eCR) LOINC code for pregnancy status (LOINC 82810-3) with its terminology bound answer codes (LOINC LL4129-4), and with SNOMED-CT terminology bindings. This code is referenced in the federally supported Family Planning Annual Report (FPAR) program and data system from HHS, which we believe should be included as a reference in version 5. The currently accepted IPS “Pregnancy Status” submission standards specifications is missing the recommended 82810-3 LOINC code in its text.
NACHC would strongly recommend that the pregnancy status data element become a component of a larger model that supports the pregnancy episode. Proposed concepts in this model are contained below. NACHC supports these formal definitions and additional women’s health data elements as components of the pregnancy episode.
Data element
DefinitionPregnancy status: Pregnancy Status = LOINC 82810-3, with its terminology bound answer codes (LOINC LL4129-4)
Indicator that patient is currently pregnant, not pregnant, or that their pregnancy status is unknown currently
Identify pregnancy episodes to help health care providers make informed decisions for the care of the patient and to inform quality improvement initiatives to improve the follow-up and documentation of peri- and postpartum care services. This data element is captured and used by providers using electronic health records or self- reported by patient as patient generated health data. However, this data is not standardized, and data exchange is not interoperable across many settings. Capturing the data related to pregnancy status in a standardized way will support the collection of sufficient pregnancy information to identify cases and measure the burden and outcomes of pregnancy on a population level.
Estimated Date of Delivery: Estimated Delivery Date (EDD) = 2.16.840.1.113762.1.4.1221.131
Date representing the expected delivery date of a pregnancy
Estimate accurate pregnancy start date to provide pregnancy information and provide key birth statistics that identify public health trends. This data element is critical for supporting maternal care coordination and care provisions. The use case will be relevant for all maternal health patients, all providers involved in maternal health care, and all consumers of maternal health data used for research, public health and patient care and quality outcomes.
Estimated Gestational Age: Age of Gestation = 2.16.840.1.113762.1.4.1221.148
The gestational age (in weeks, or weeks and fraction of week) of the pregnancy at time of pregnancy outcome
Estimate due date to inform obstetrical care and testing and evaluate the fetal growth and infant’s health at birth. The use case will be relevant for all maternal health patients and infants, all providers involved in maternal and infant health care, and all consumers of maternal and newborn health data used for research, public health and patient care and quality outcomes.
Gravidity: [#] Pregnancies = LOINC 11996-6
Total number of times the patient has been pregnant including the present pregnancy. This element supports obstetric risk and patient history.
Parity: [#] Parity = LOINC 11997-6
Total number of times the uterus has been emptied of viable offspring.
The outcome of the pregnancy: 1) live birth; 2) still birth or intrauterine fetal death (>20 weeks gestation); 3) miscarriage/spontaneous abortion (<20 weeks gestation); 4) termination (elective, medical, surgical, or induced abortion); 5) ectopic pregnancy; 6) non-live birth, not otherwise specified
Document pregnancy outcomes to assess care processes and develop effective approaches to maternal care. Linkages between mother and infant records will also be beneficial for clinical care as well as for public health (important to link data on mothers and infants especially for diseases such as Zika, Hep B, and others). This data is also routinely exchanged for birth certification, fetal death reporting, and birth defect reporting. Standardization will benefit the data exchange between EHR systems and public health, specialized registries, national health care survey systems, and research entities.
Date of pregnancy outcome:
Date when an event occurred relative to pregnancy outcome. This concept links to the actual date of delivery or any other pregnancy outcome and would be the element generated as a pregnancy episode is closed.
Document date of when the pregnancy outcome occurred. The use case will be relevant for all maternal health patients, all providers involved in maternal health care, and all consumers of maternal health data used for research, public health and patient care and quality outcomes.
Pregnancy complications: Complications of Pregnancy, Childbirth and the Puerperium = 2.16.840.1.113883.3.464.1003.111.12.1012
Complications of pregnancy that include physical and mental conditions that affect the health of the pregnant or postpartum person, the infant, or both.
Identify adverse pregnancy complications that can have lifelong effects on the pregnant individual’s health, such as developing hypertension or cardiovascular disease post-delivery, as well the infant’s health. The use case will be relevant for all maternal health patients, all providers involved in maternal health care, and all consumers of maternal health data used for research, public health and patient care and quality outcomes.
Postpartum status:
The time period after delivery up to 12-months
Identify time period subsequent to pregnancy episode and patients who should receive specific postpartum care services. The use case will be relevant for all maternal health patients, all providers involved in maternal health care, and all consumers of maternal health data used for research, public health and patient care and quality outcomes.
NACHC also recommends the consideration of additional concepts (Value sets available in VSAC)
Postpartum care visit
Postpartum care visit (occurring within 3-12 weeks after delivery)
Increase the proportion of all postpartum patients who receive initial postpartum care from -their obstetrician–gynecologists or primary care providers based on current or existing guidance and recommendations. Underutilization of postpartum care impedes management of chronic conditions, such as mental health, diabetes, hypertension, and obesity, and access to effective contraction, which increases the risk of short interval pregnancy and preterm birth. The use case will be relevant for all maternal health patients, all providers involved in maternal health care, and all consumers of maternal health data used for research, public health and patient care and quality outcomes.
Postpartum care visit quality services
Provide evidence-based quality postpartum care services at visit: 1) contraceptive counseling and provision of a contraceptive method (LOINC 86654-1); 2) postpartum depression screening within 8 weeks of delivery (LOINC 89211-7); 3) postpartum depression treatment for those diagnosed with postpartum depression (LOINC 71354-5); 4) postpartum diabetes screening for women with GDM-affected pregnancy; 5) pregnancies with chronic or gestational hypertension (ICD 10 O13.9; 6) pregnancies with hypertension in pregnancy and subsequent preeclampsia (ICD 10 O14.95), eclampsia (ICD 10 O14.90) and HELLP syndrome (ICD-10 code O14.24) outcomes; 7) breastfeeding (LOINC 63895-7); 8) infant feeding and care; and 9) other evidence-based recommendations for postpartum care services
Track postpartum care service provision to reduce gaps in care and improve adherence to evidence-based guidelines. The use case will be relevant for all maternal health patients and infants, all providers involved in maternal health care, and all consumers of maternal health data used for research, public health and patient care and quality outcomes.
Delivery Encounters
A set of standardized delivery encounters could be used to trigger automated structured ADT messages already required by CMS at the beginning and the end of the encounter. Reuse of well constructed code sets from deployed quality measures can assist in care coordination.
There is a critical need for expanded standardized data elements for the documentation of reproductive health care. This expansion can increase attention to and standardize reporting of this aspect of medical care. Patient-centered prefererences are challenging to capture and share because of the lack of interoperable data standards to support their standardized use. NACHC participated in the development of the SINC data element using a human-centered design approach led by health center care teams and with industry experts on contraceptive and reproductive health care. We encourage ONC to add additional patient preferences supporting reproductive care to USCDI and USCDI+.
There is a documented gap in access to contraceptive services for people of reproductive age. Even when patients receive other types of health services, their pregnancy prevention needs often go unmet.
SINC is a standardized screening tool which can help providers center their patients’ reproductive health preferences and needs, using a service-needs screening question. SINC is unique in its approach, as other recognized contraceptive care screening questions counsel patients through a pregnancy-intention frame, which makes assumptions about a patient’s desire for contraceptive use based on their feelings around becoming pregnant within a calendar year.
Research has shown that patients prefer a service-needs approach when being asked about their reproductive health needs, as this area of healthcare can be sensitive and highly stigmatized within communities. SINC centers patient autonomy by giving patients the space to identify their needs, rather than making assumptions and directing them towards a certain outcome.
Centering patient autonomy in the reproductive healthcare space is critical, as there is a long history of reproductive coercion and oppression in the United States.
SINC was created and optimized for the primary care setting but can be used in a variety of care settings.
SINC is included in FPAR 2.0, the new set of data elements for federal reporting of the Title X program, administered by the Office of Population Affairs (OPA)
SINC is used as part of an electronic clinical quality measure (eCQM) of contraceptive access, which has been endorsed by the National Quality Forum (NQF) and Partnership for Quality Measurement (PQM). SINC refines the denominator of the eCQM, ensuring patients who have indicated that they do not have interest in contraceptive use are excluded from the calculation.
SINC is currently available for use in several EHR systems, such as OCHIN Epic and eClinical Works, and is currently being used by large healthcare organizations and health departments, including Planned Parenthood and multiple large municipal health departments. NACHC worked with a sample of health centers using different EHR systems across the country and users reported this element did add to their ability to document the patient's preferences and to utilize that data to improve care.
Use of SINC in health centers continues to grow. In 2023, nine community health center networks (CHCs), located across the continental United States, piloted SINC as part of a nine-month quality improvement learning collaborative. Approximately 9,000 SINC responses were recorded in EHR systems as part of this project.
SINC is designed to be used as part of patient-centered clinical workflows and has been found to be feasible and acceptable by health care teams. The use of this element without the presence of documentation of a recent contraceptive service or counseling should be used to assist care teams in identifying patients who may be interested and in need of contraceptive services.
CSTE continues to support pregnancy status as included data element in USCDI v5. However, a single variable is not sufficient to capture critical data that are needed for a large variety of conditions affecting the public's health, including maternal mortality, Hepatitis B and C, COVID-19, Zika, syphilis, and influenza, to name only a few. Additionally, the data element description, which includes intent to become pregnant, should be revised to be simply 'current pregnancy status' - indicating whether the person is pregnant, not pregnant, or unknown.
6) Postpartum status (this is important since if the mother recently gave birth and is diagnosed with a condition that could affect the neonate, public health action might be indicated).
Currently there are large gaps in the ability for data from electronic health records or ELR to capture sufficient pregnancy information to identify cases and measure the burden and outcome of medical conditions and infections in pregnancy on a population level. Standardizing these data for exchange would be a substantial step forward.
CSTE strongly urges ONC to include Estimated due date and not just gestational age as an element in USCDI since data are exchanged at points in time and gestational age at the time of recording may differ from gestational age at the time of the data transmission or receipt. Including estimated due date fixes the maturity of the pregnancy in time, as opposed to gestational age. If gestational age is favored as a variable to use then it must be accompanied by a date of recording of the gestational age which requires additional data capture.
Finally, it is very important for electronic health records to develop a way to link the mother and infant records. A unique identifier for the mother which can be included in the infant's record, and a similar unique identifier for the infant which can be included in the mother's records would help to rectify this problem, which would be beneficial for both clinical care as well for public health when we receive data on mothers and infants but cannot link them (important for diseases such as HIV, listeria, Zika, syphilis, Hepatitis B, and others).
Pregnancy Status and Outcome are critical fields which must be included in USCDI v5. Pregnancy Status and Outcome are critical for prioritization of public health actions and without this information adverse outcomes may occur. Many conditions of public health importance can result in spontaneous abortion, prematurity, or fetal death. CSTE stresses the importance of restricting access or sharing of reproductive health data to ensure it cannot be used for purposes beyond the immediate public health purpose for which it was reported.
CDC supports the inclusion of this data element in USCDI v5 as it is an element that may be necessary for calculation of our digital quality metrics from FHIR data.
When the Pregnancy Information Data Element Class is added, consider moving this data element to Pregnancy Information Data Element Class.
Consider having NIH NCI EVS manage/provide guidance into the data element classes and hierarchy. The classes seem to mimic a healthcare chart which in some cases has redundancies that are historical in nature from the way things were done in the paper world with paper charts. Back in the day, we had tabs, we put things (the chart sections labaled much like these data classes) where they made sense to us (it was standardized if you were fortunate enough to have a secretary who organized it for you). Now with the ontologies and technological capabilities, the information can be placed in the appropriate hierarchical branch of health science ontology. Thank you.
Support - LOINC 82810-3 mirrors HL7 14.66.1. Enabling either value set will provide a potential for greater data capture and more information would be available to LHDs.
There is an important distinction regarding the IHE specifications, specifically LOINC 10162-6 "History of pregnancies Narrative". This note captures the historical context of pregnancies rather than the current pregnancy episode status of the patient. We recommend transparency in utilizing standard terminology and codes that accurately represent pregnancy status at the patient level, emphasizing structured data as endorsed by various HL7/FHIR IGs and implemented by government agencies, academic institutions, and community health centers.
Please align this data element's specifications with the electronic case reporting (eCR) LOINC code for pregnancy status (LOINC 82810-3) along with SNOMED-CT terminology bindings. The preferred reference should be the pregnancy status LOINC 82810-3, coupled with its associated answer codes (LOINC LL4129-4).
These codes are integral to the federally supported Family Planning Annual Report (FPAR) program and data system by HHS, which we advocate for inclusion in the version 5 draft.
Moreover, NACHC stands in alignment with CDC and ACOG’s positions in endorsing HL7’s CCDA “Pregnancy Status” and related women’s health data elements, recognizing it as a distinct data class as outlined in Appendix C of the attached document.
CSTE continues to support pregnancy status as included data element in USCDI v5. However, a single variable is not sufficient to capture critical data that are needed for a large variety of conditions affecting the public's health, including maternal mortality, Hepatitis B and C, COVID-19, Zika, syphilis, and influenza, to name only a few. CSTE urges the inclusion of the following variables in the core data for exchange - as defined by the ONC Public Health Task Force on Capturing Pregnancy Data in Electronic Health Records and found here https://www.healthit.gov/sites/default/files/facas/HITJC_PHTF_Meeting_Slides_2017-03-30_0.pdf
https://www.healthit.gov/topic/federal-advisory-committees/collaboration-health-it-policy-and-standards-committees (See May 19 transmittal letter to the NC. Click on charge 1 - Capturing Pregnancy Status, see MS Excel Spreadsheet)
Pregnancy Status - Yes, No, Possible, Unknown
Date pregnancy status recorded
Estimated delivery date
Pregnancy outcome
Date of pregnancy outcome, and optionally
Postpartum status (this is important since if the mother recently gave birth and is diagnosed with a condition that could affect the neonate, public health action might be indicated).
Currently there are large gaps in the ability for data from electronic health records or ELR to capture sufficient pregnancy information to identify cases and measure the burden and outcome of medical conditions and infections in pregnancy on a population level. Standardizing these data for exchange would be a substantial step forward.
Finally, it is very important for electronic health records to develop a way to link the mother and infant records. A unique identifier for the mother which can be included in the infant's record, and a similar unique identifier for the infant which can be included in the mother's records would help to rectify this problem, which would be beneficial for both clinical care as well for public health when we receive data on mothers and infants but cannot link them (important for diseases such as HIV, listeria, Zika, syphilis, Hepatitis B, and others)
The "Optional Background Text / Cover Letter" field provides space for additional context or introductory information related to your comment.
If you wish to provide context, explanation, or an introduction to your comment, enter this information in the field labeled "Optional Background Text / Cover Letter." This is entirely optional and is most useful when submitting multiple related comments or when additional background would help reviewers understand your feedback.
If you are only commenting on a single data class or element, you may leave this field blank.
2. Select the Data Class
To specify which data class your comment addresses:
In the "Data Class" drop-down menu, select the appropriate data class you want to comment on.
If you are providing a general comment that is not specific to a data element, select "General" from the options. Comments with this designation will be displayed on the USCDI landing page.
Note that the Data Class field will automatically populate based on your current location in the platform:
If you are on a data class page, the field will be set to that specific data class
If you are on a data element page, the corresponding data class will be pre-selected
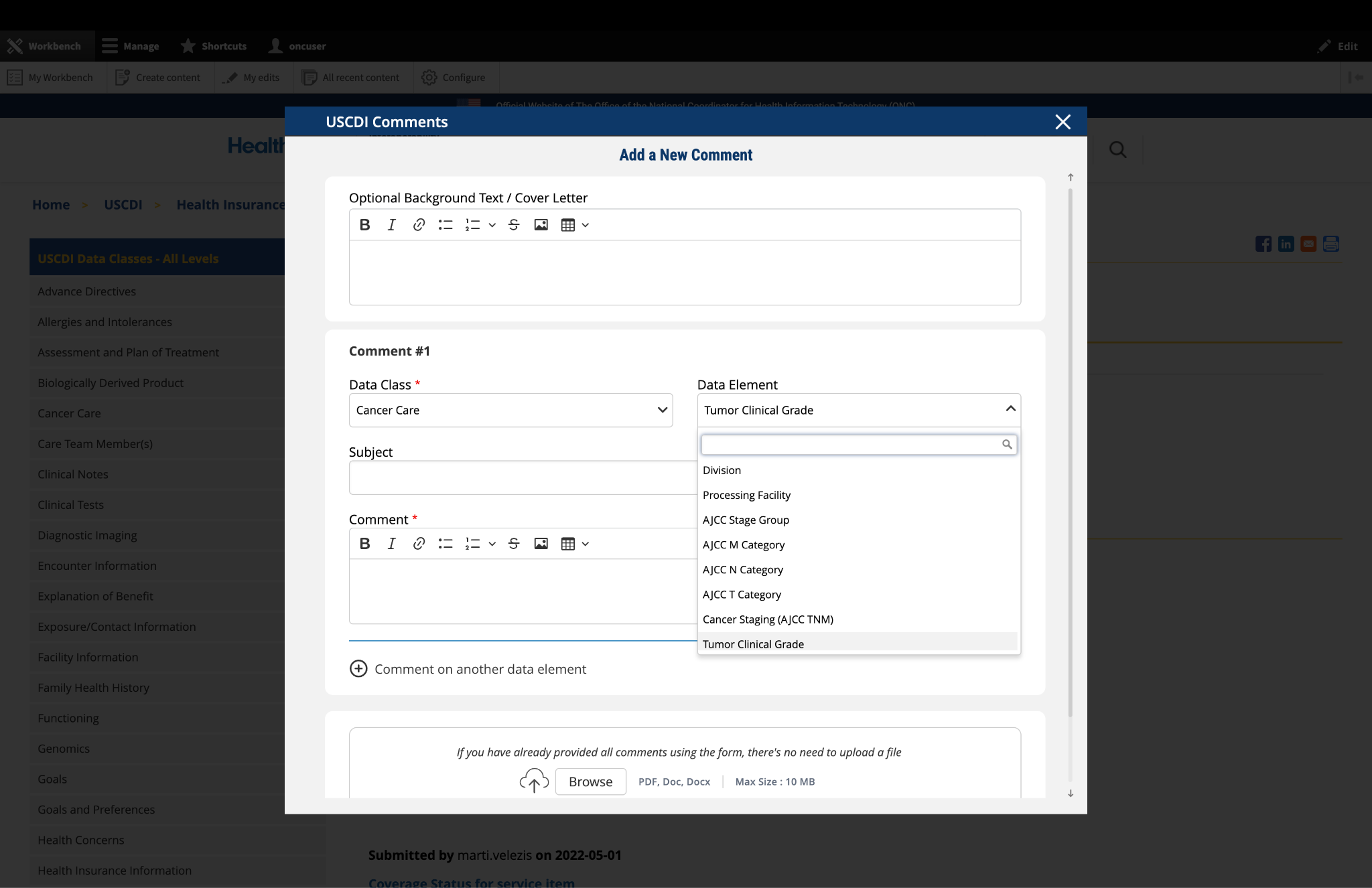
3. Select the Data Element
To specify which data element your comment addresses:
In the "Data Element" drop-down menu, select the specific data element you want to comment on.
The drop-down menu will display only the elements available under the data class you selected in the previous step.
You can use the search function within the drop-down to quickly locate a specific data element.
If you are commenting on the data class itself rather than a specific element, you may leave this field blank.
Note: Comments on a specific data element will appear on the respective data element page, while comments on a data class (without a specific element selected) will appear on the landing page for that data class.
Fig 1 The "Data Class" and "Data Element" dropdown menus allow users to specify the exact content they wish to comment on.
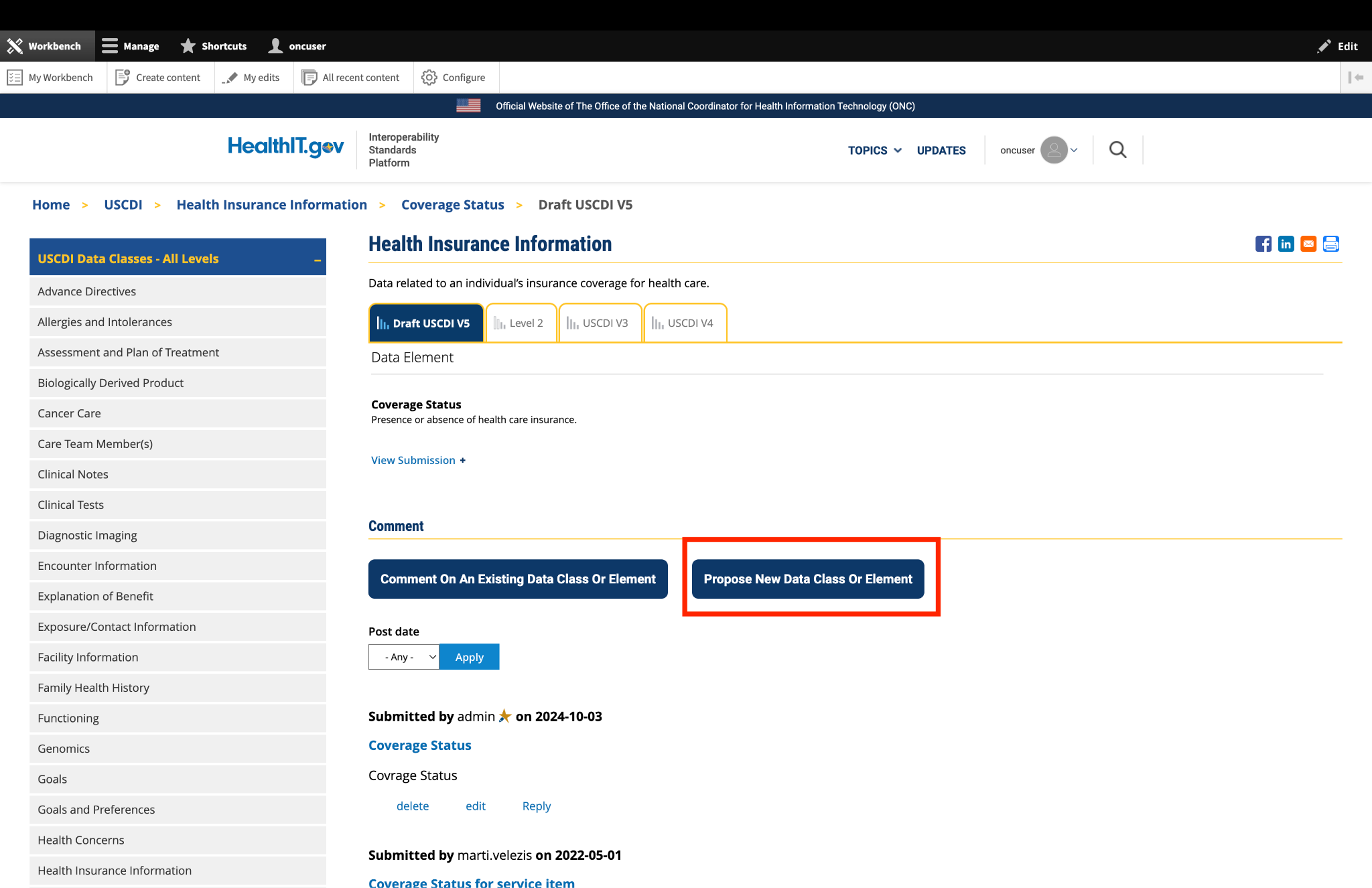
4. Optional: Propose New Data Class or Element
If you cannot find the appropriate data class or element for your comment:
Instead of clicking the "Comment On An Existing Data Class Or Element" button, click the adjacent button labeled "Propose a New Data Class or Data Element."
This will redirect you to the ONDEC (ONC New Data Element and Class) Submission System.
In the ONDEC system, follow the provided instructions to submit your proposal for a new data class or element.
Once your proposal is submitted through ONDEC, it will be reviewed separately from the commenting process.
Fig 2 The "Propose a New Data Class or Data Element" button redirects users to the ONDEC Submission System for proposing new data elements not currently available in the system.
5. Complete the Comment Form
Fill out the required fields in the comment form:
Subject: Enter a brief, descriptive title that summarizes your comment. This helps reviewers quickly understand the nature of your feedback.
Comment: In this field, provide the full details of your comment or feedback. Be as clear and specific as possible about your suggestions, concerns, or observations. Include any relevant details that support your position.
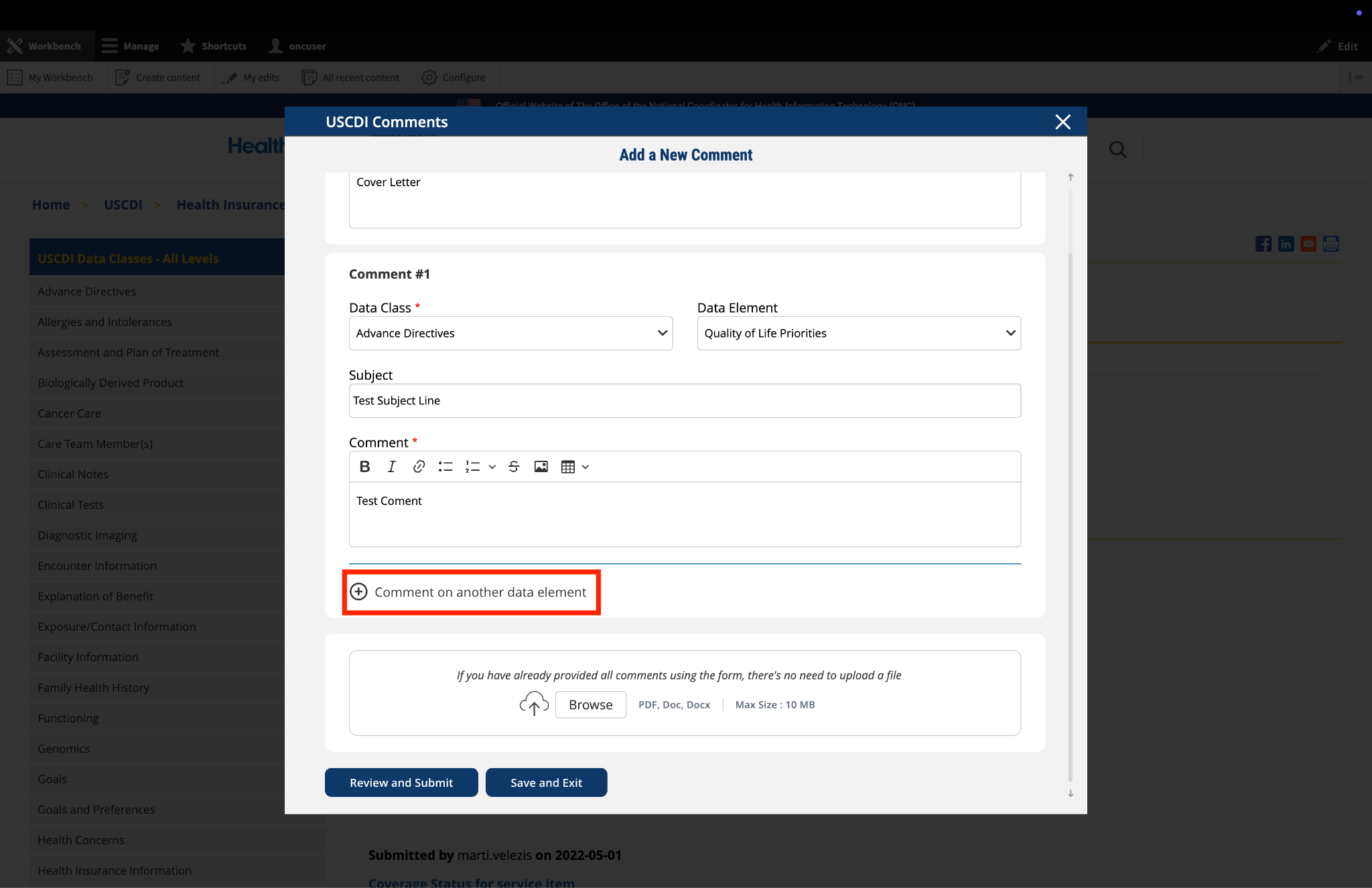
6. Optional: Add Additional Comments
If you need to comment on multiple data classes or elements:
After completing your first comment, click the link labeled "Comment on another data element" at the bottom of the form.
A new comment section will appear, allowing you to enter details for your additional comment.
For each additional comment, you must select the appropriate data class and data element from the drop-down menus.
Complete the Subject and Comment fields for your additional comment.
Repeat this process for each additional comment you wish to submit.
Fig 3 The "Comment on another data element" link enables users to create multiple comments addressing different elements within a single submission.
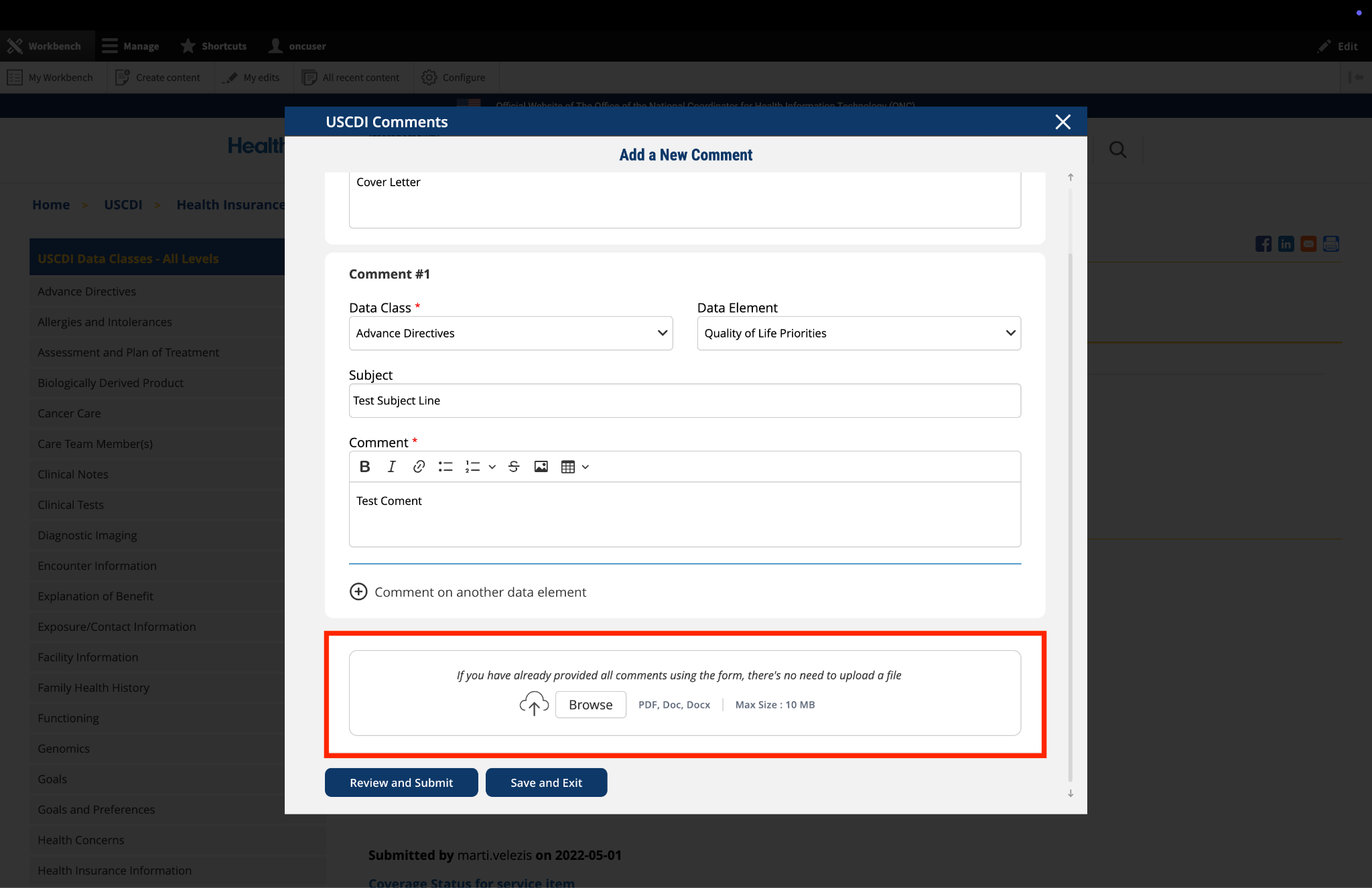
7. Optional: Upload Supporting Files
The platform allows you to upload supporting documentation to enhance your comment:
Locate the "File Upload" section at the bottom of the comment form.
Click to upload any files (such as PDFs or documents) that provide additional context, evidence, or clarification for your comment.
Important: If you have already entered your comments using the form fields, there is no need to upload duplicate content in PDF format. The file upload feature is intended for supplementary materials only. Please avoid uploading files that contain the same information already provided in your comment text.
Fig 4 The "File Upload" section permits users to attach supporting documentation that supplements their written comments.
8. Optional: Save and Exit
If you need to pause your work and return to complete your comment later:
Click the "Save and Exit" button at the bottom of the form.
Your comment will be saved as a draft that you can access and complete later.
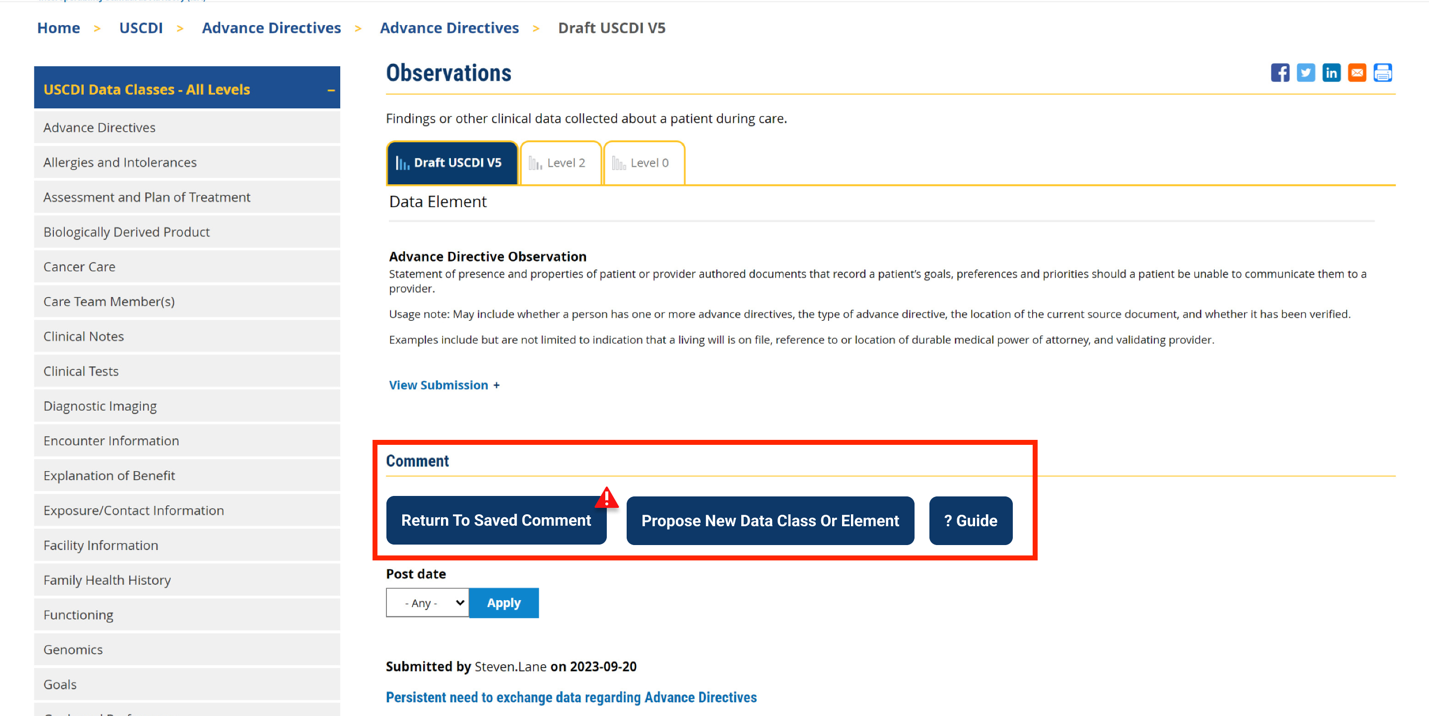
When you return to the platform, you will see a red triangle with an exclamation mark next to the “Return to saved Comment” button, indicating that you have saved comments in draft status.
Click this button to continue working on your draft.
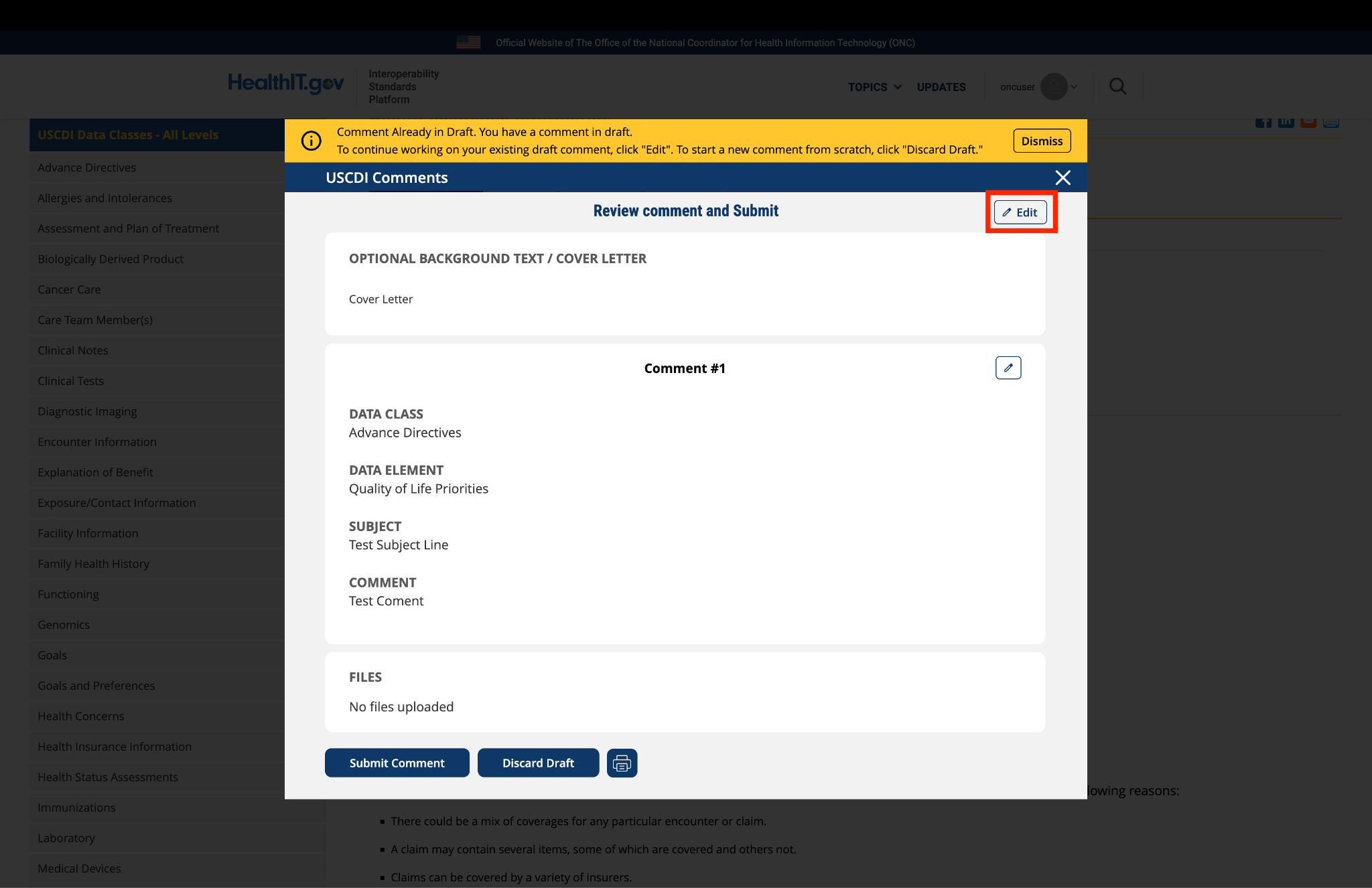
You will be taken to a review page where you can:
Select "Submit Comment" to officially submit your feedback.
Click "Edit" to return to the comment form and make changes
Select "Discard Draft" to delete the saved draft and start fresh
Fig 5 A red triangle with exclamation mark indicator appears next to the “Return to saved Comment” button when draft comments are saved in the system.
9. Review and Submit
Once you have completed your comment:
Click the "Review and Submit" button at the bottom of the form.
This will take you to a review screen displaying your comment(s) in full.
Review all information for accuracy and completeness.
On this review screen, you have three options:
Click "Submit Comment" to officially submit your feedback
Click "Edit" to return to the comment form and make changes
Click "Discard Draft" to delete the comment and start fresh
The review screen also includes a "Print" button that allows you to create a printed copy of your comments for your records.
If you choose to submit, your comment will be recorded in the system and made available for review by the appropriate stakeholders.
Fig 6 The review screen allows users to verify comment content and make any necessary modifications before final submission.


Submitted by BLampkins_CSTE on
Pregnancy Status - CSTE Comment