
Submitted by BLampkins_CSTE on
CSTE Comment - v6
CSTE supports inclusion of this data element in USCDI V6. Please see previously submitted CSTE comments for additional recommendations.
 Official Website of the Office of the National Coordinator for Health Information Technology
Official Website of the Office of the National Coordinator for Health Information Technology
Data Element |
||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Estimated Date of Delivery
|
||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||
Submitted by BLampkins_CSTE on
CSTE supports inclusion of this data element in USCDI V6. Please see previously submitted CSTE comments for additional recommendations.
Submitted by CDC_DSMH_WG on
CDC requests this data element be considered for inclusion in USCDI V6. A recent CDC/NACHC postpartum care services project documented the feasibility of collecting the data element in EHRs, and the importance for interoperability standards to support data exchange between health organizations to enhance quality improvement initiatives to improve perinatal outcomes.
Justification: Estimated Date of Delivery is the date representing the expected delivery date of a pregnancy. It is a physician's best estimate of the date of delivery and is determined at the initial diagnosis of pregnancy and can be confirmed by an ultrasound, physical exam, or last menstrual period. This data element is critical for helping health care providers make informed decisions for the care of the patient (such as timing for recommended screenings and vaccinations), supporting maternal care coordination and care provision, and developing data and clinical care quality improvement initiatives. For data and clinical care quality improvement initiatives to be successful, there needs to be standardized documentation and follow-up based on stage of pregnancy and notifications for when postpartum care should begin. Despite the importance of data to successfully identify, treat, and follow up with patients, critical data on pregnancy status and pregnancy outcomes are not standardized across electronic health records (EHRs). The use case will be relevant for all maternal health patients, all providers involved in maternal health care, and all consumers of maternal health data used for research, public health and patient care and quality outcomes.
The Centers for Disease Control and Prevention, in partnership with the National Association of Community Health Centers (NACHC), worked to build capacity of Federally Qualified Health Centers to improve the health informatics infrastructure for perinatal care measures and use perinatal care measures to identify and address gaps in postpartum care (https://liebertpub.com/doi/10.1089/jwh.2024.0364). Partner health center-controlled networks (Alliance Chicago, Health Choice Network, OCHIN, and Aliados Health) and nine Community Health Centers, implemented strategies to integrate evidence-based recommendations into the clinic workflow and use data-driven health information technology (HIT) systems to improve data standardization for quality improvement of postpartum care services. The respective EHRs were able electronically capture, access and exchange this data element through adequate testing in staging and development EHR environments. NACHC has developed an implementation Guide (Improving Quality in Pregnancy and Postpartum Care to provide practical strategies to leverage data from electronic clinical data systems for improved maternal health care (NACHC-WHPP-Implementation-Guide-2024_3.pdf).
This data element is captured as active in Logical Observation Identifiers Names and Codes (LOINC®) ontology as: 11780-4: Delivery date Estimated from ovulation date, a quantitative scale type and 57060-6: Estimated date of delivery Narrative, a narrative scale type.
EDD is also captured in the Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) as 161714006 and 738070007.
Interoperability in the clinical space is key to optimizing many processes including the diagnosis, management, and transition of care from obstetricians to primary care clinicians for people with hypertensive disorders of pregnancy. Accurately capturing active pregnancies, their ultimate outcomes, and pertinent dates is a major challenge within electronic health records (EHRs). This has at least a two-fold potential negative impact: 1) people may not receive the guideline-recommended care they need during their pregnancy and postpartum phases and 2) women may appear to be continuously pregnant for multiple years in EHRs. Below is some additional information for consideration:
An exploration of IQVIA Ambulatory Electronic Medical Record (AEMR) data demonstrates that estimated delivery date is not universally captured for pregnant patients, even within OB/GYN practices. In IQVIA AEMR data from 2022-2023, CDC identified pregnant patients using a complex algorithm* that incorporates five types of measures: diagnoses, measurements, observations, procedures, and drugs. When CDC examined pregnant patients being treated by all types of clinical providers, of 34,238 pregnant patients, 10,614 (31%) had an observation that specified estimated delivery date. When CDC examined pregnant patients being treated by OB/GYN providers, of 6,583 pregnant patients, 3,848 (58.5%) had an observation that specified estimated delivery date. Thus, even among OB/GYN providers, more than 40% of patients identified as being pregnant through the comprehensive pregnancy electronic phenotype* did not have an EDD in their EHR. Moreover, the capture of EDD is not standardized across EHRs of clinical providers contributing data to IQVIA and the native data have to be mapped into 5 OMOP observations:
These findings speak to the need to include Estimated Delivery Date as a required USCDIv6 data element to provide a standardized, universally captured data point that allows for the characterization of pregnancy and calculation of gestational age (both of which have widespread implications for clinical practice across specialties).
*Matcho A, Ryan P, Fife D, Gifkins D, Knoll C, Friedman A. Inferring pregnancy episodes and outcomes within a network of observational databases. PLoS One. 2018 Feb 1;13(2):e0192033. doi: 10.1371/journal.pone.0192033.
Submitted by CDC_DSMH_WG on
Submitted by CDC_DSMH_WG on
Proposed change:
NACCHO supports removing this from the Estimated Delivery Date data element, but this should be kept in some form (either as a new data element or under another term). These details are critical to LHDs understanding what preventative programs they need to put into place to ensure a supported pregnancy and reduce negative newborn outcomes.
Submitted by CDC_DSMH_WG on
CDC Supports inclusion of this data element in USCDI v5.
Submitted by CDC_DSMH_WG on
CSTE Comment:
Submitted by CDC_DSMH_WG on
CSTE Comment:
Submitted by CDC_DSMH_WG on
Submitted by CDC_DSMH_WG on
General Comment: Recommend moving this element to a new Mother's Pregnancy Information USCDI Class (not in the Observation class).
The "Optional Background Text / Cover Letter" field provides space for additional context or introductory information related to your comment.
If you wish to provide context, explanation, or an introduction to your comment, enter this information in the field labeled "Optional Background Text / Cover Letter." This is entirely optional and is most useful when submitting multiple related comments or when additional background would help reviewers understand your feedback.
If you are only commenting on a single data class or element, you may leave this field blank.
To specify which data class your comment addresses:
To specify which data element your comment addresses:
Note: Comments on a specific data element will appear on the respective data element page, while comments on a data class (without a specific element selected) will appear on the landing page for that data class.
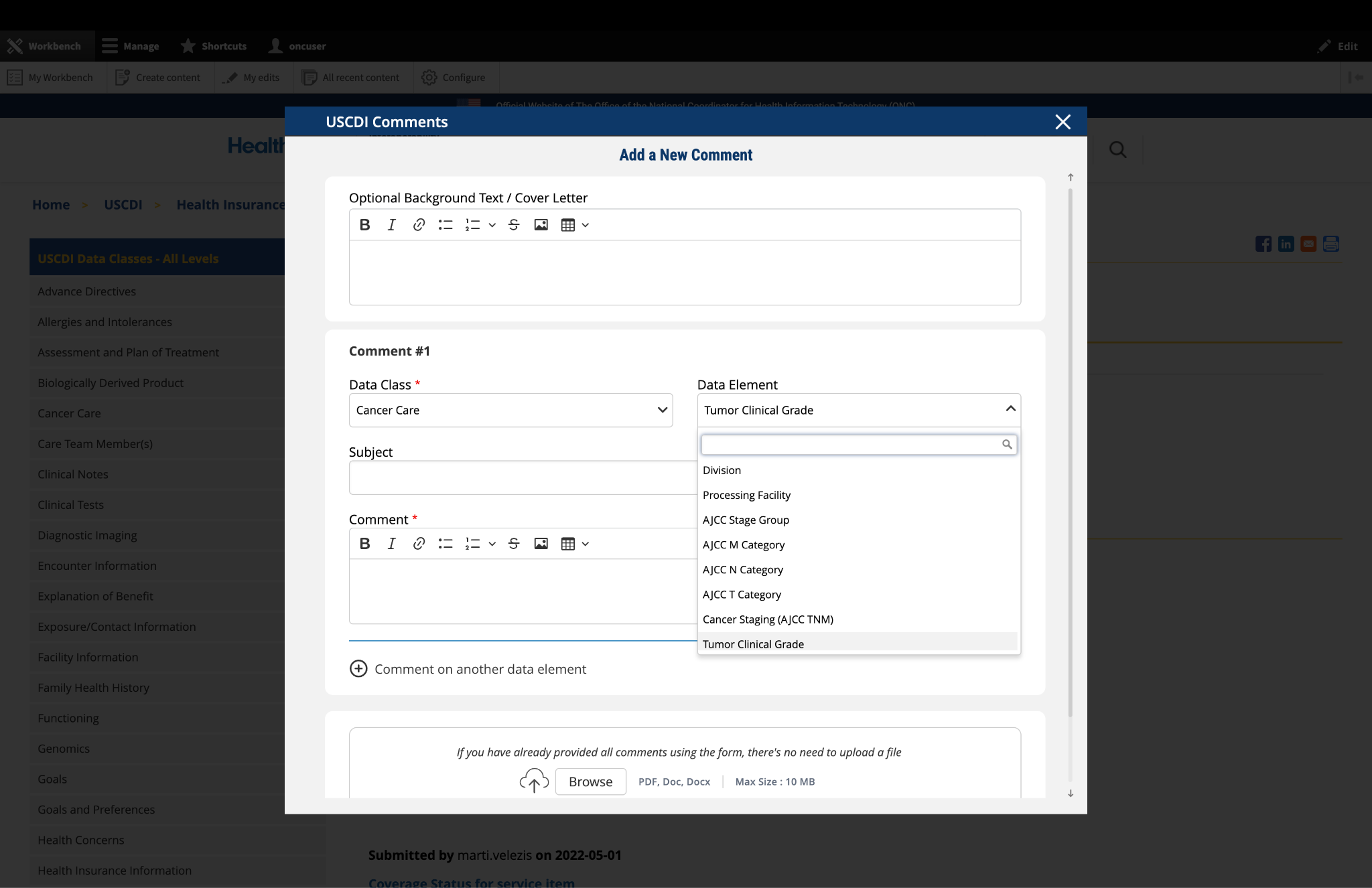
Fig 1 The "Data Class" and "Data Element" dropdown menus allow users to specify the exact content they wish to comment on.
If you cannot find the appropriate data class or element for your comment:
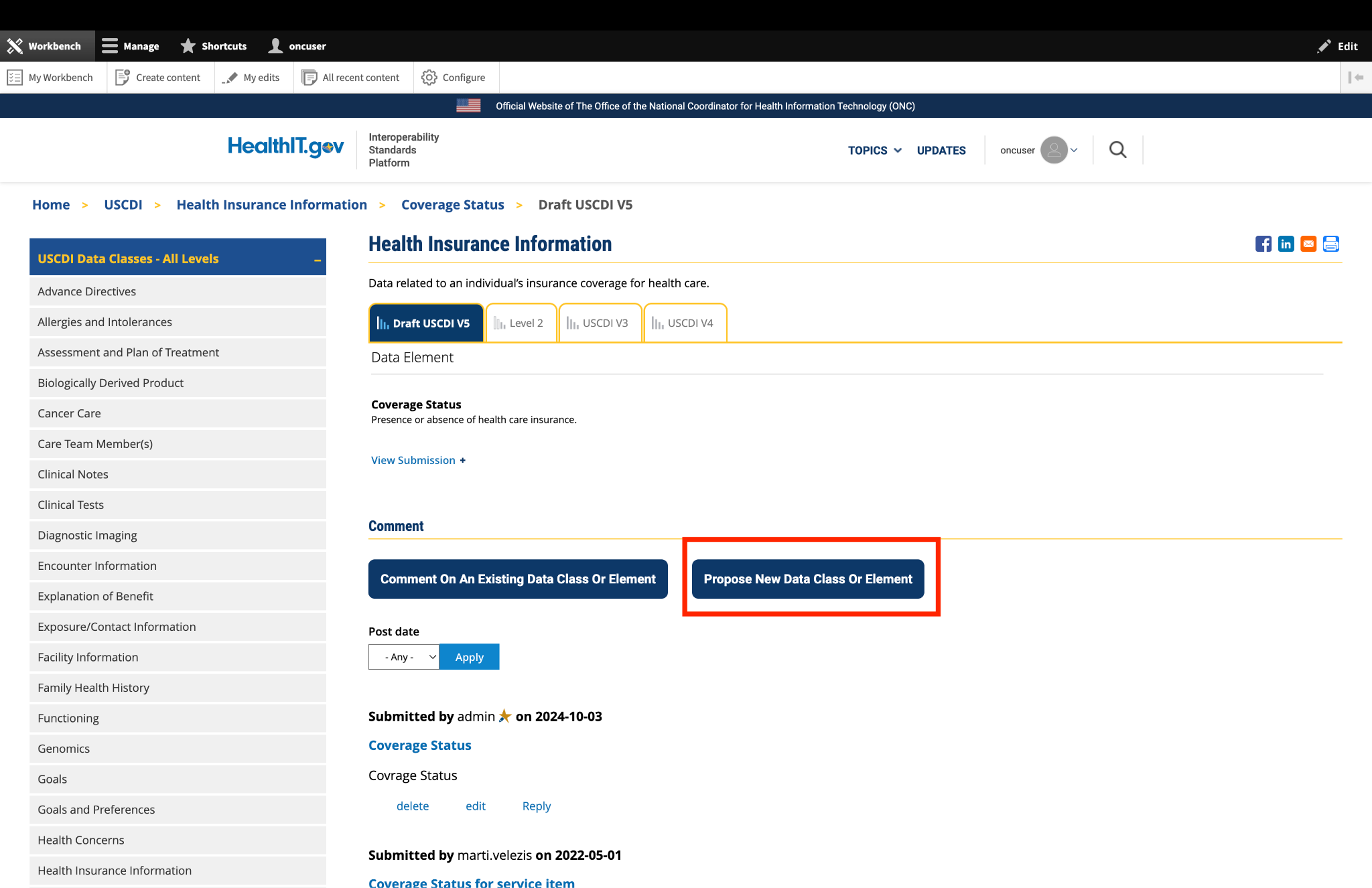
Fig 2 The "Propose a New Data Class or Data Element" button redirects users to the ONDEC Submission System for proposing new data elements not currently available in the system.
Fill out the required fields in the comment form:
Subject: Enter a brief, descriptive title that summarizes your comment. This helps reviewers quickly understand the nature of your feedback.
Comment: In this field, provide the full details of your comment or feedback. Be as clear and specific as possible about your suggestions, concerns, or observations. Include any relevant details that support your position.
If you need to comment on multiple data classes or elements:
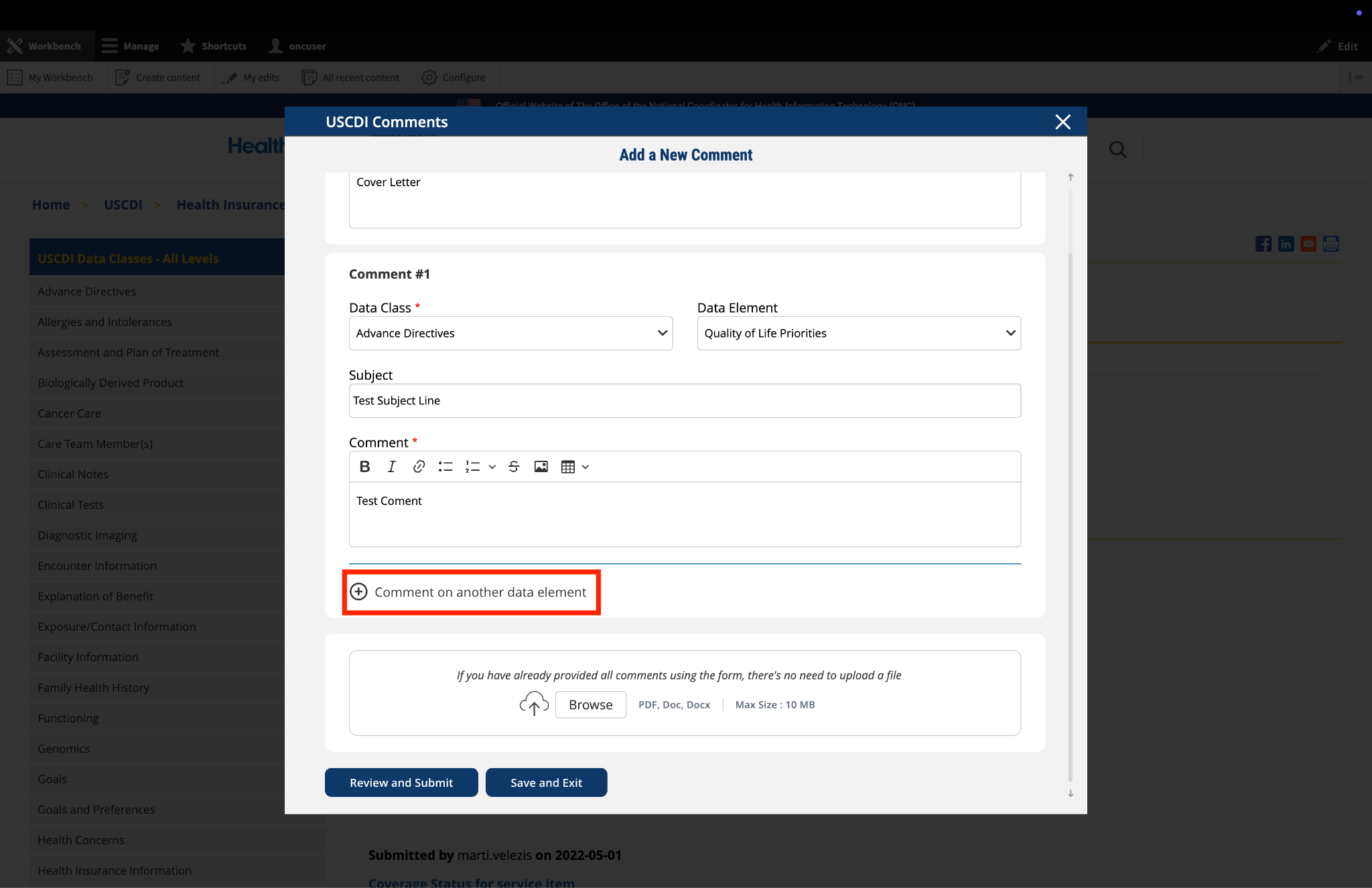
Fig 3 The "Comment on another data element" link enables users to create multiple comments addressing different elements within a single submission.
The platform allows you to upload supporting documentation to enhance your comment:
Important: If you have already entered your comments using the form fields, there is no need to upload duplicate content in PDF format. The file upload feature is intended for supplementary materials only. Please avoid uploading files that contain the same information already provided in your comment text.
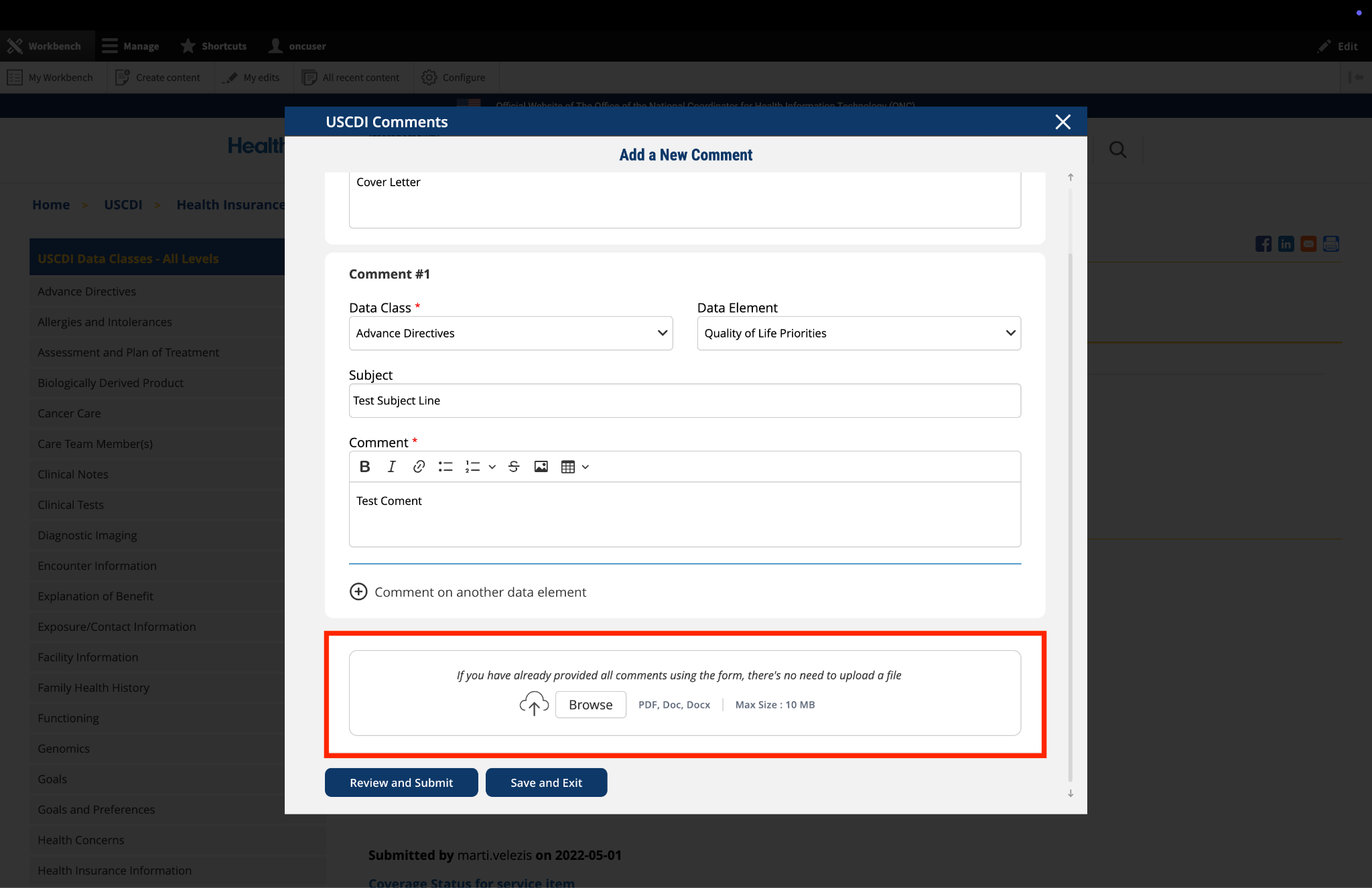
Fig 4 The "File Upload" section permits users to attach supporting documentation that supplements their written comments.
If you need to pause your work and return to complete your comment later:
Fig 5 A red triangle with exclamation mark indicator appears next to the “Return to saved Comment” button when draft comments are saved in the system.
Once you have completed your comment:
Fig 6 The review screen allows users to verify comment content and make any necessary modifications before final submission.
Submitted by minigrrl on
What is the justification…
What is the justification for the demotion of the following Case Reporting data elements in USCDI, specifically:
• Exposure/Contact Information: Exposure/Contact Agent
• Exposure/Contact Information: Exposure/Contact Date
• Exposure/Contact Information: Exposure/Contact Direction
• Exposure/Contact Information: Exposure/Contact Source/Target Participant
• Exposure/Contact Information: Exposure/Contact Type
• Health Insurance Information: Medicare Patient Identifier
• Immunizations: Vaccination Administration Date
• Laboratory: Specimen Collection Date/Time
• Patient Demographics/Information: Patient Birth Place
• Patient Demographics/Information: Tribal Enrollment
• Pregnancy Information: Estimated Date of Delivery
• Pregnancy Information: Gestational Age
• Pregnancy Information: Last Menstrual Period (LMP)
• Provenance: Unique Identifier
• Social Determinants of Health: Housing Instability and Homelessness
• Social History: Congregate Living
• Work Information: Employment Status
• Work Information: Job Employer Address
• Work Information: Job Employer Name
• Work Information: Usual Industry
• Work Information: Usual Occupation
Currently, 21 certified EHR products exchange these elements using electronic Case Reporting (eCR) specifications demonstrating real-world adoption that typically supports promotion, not demotion, within the USCDI maturity model.
Collectively, these elements provide clinical, demographic, occupational, social, and epidemiological context essential to disease investigation and outbreak response for nationally notifiable conditions.
We urge ONC to either reverse this decision or publish a detailed, evidence-based rationale.