Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Represents information or details about an individual's physical, cognitive, intellectual, or psychiatric disabilities.
Use Case Description(s)
Use Case Description
Individuals living with disabilities face barriers to receiving proper medical care when their doctors and care teams are not aware of existing disabilities. Consequently, these barriers exacerbate health disparities and result in inferior care and poor outcomes. Appointments may need to be rescheduled, care may not be coordinated properly, breakdowns in communication and trust will also negatively impact patient care without carefully documenting disability status. If properly documented, an alert could notify appropriate care team members and staff to address any physical access barriers, arrange for interpreters, plan for various forms of communication and patient support tools.
Applications for disability benefits could be further automated and streamlined with the addition of this data element.
If we are going to improve the lives and care of individuals living with disabilities, we must prioritize capturing and sharing this data accordingly.
Estimate the breadth of applicability of the use case(s) for this data element
Not currently captured or accessed with an organization
Extent of exchange
N/A
Potential Challenges
Restrictions on Standardization (e.g. proprietary code)
Unknown
Restrictions on Use (e.g. licensing, user fees)
Unknown
Privacy and Security Concerns
Unknown
Estimate of Overall Burden
Unknown
ASTP Evaluation Details Each submitted Data Element has been evaluated based on the following criteria. The overall Level classification is a composite of the maturity based on these individual criteria. This information can be used to identify areas that require additional work to raise the overall classification level and consideration for inclusion in future versions of USCDI
Criterion #1 Maturity - Current Standards
Level 2 - Data element is represented by a terminology standard or SDO-balloted technical specification or implementation guide.
Criterion #2 Maturity - Current Use
Level 0 - Data element is captured, stored, or accessed in limited settings such as a pilot or proof of concept demonstration.
Criterion #3 Maturity - Current Exchange
Level 0 - Data element is electronically exchanged in limited environments, such as connectathons or pilots.
Criterion #4 Use Case(s) - Breadth of Applicability
Level 1 - Use cases apply to several care settings or specialties.
Submitted By: James Patterson
/ PACIO Project
Data Element Information
Data Element Description
A self-reported status that identifies individuals with disabilities or conditions that impact major life activities, used to ensure equal access and may inform accommodation needs.
Examples include, but are not limited to, the required responses for the American Community Survey six-question set (ACS-6) and optional capture of other surveys such as the Washington Group Short Set on Functioning (WG-SS).
Rationale for Separate Consideration
The USCDI “Disability Status” data element (for which we recommend USCDI change its name to “Disability Assessment”), currently encapsulates both (1) demographic information, which is used to support population-level health surveillance and accommodation access, and (2) individual-level patient information, which is used to inform clinical decisions. These are two different and distinct types of data used for different purposes, with the population-level demographic data being defined using the “Disability Status” name and the individual-level patient information not aligned with the idea of a disability status.
The distinct difference between these two different types of data encapsulated in the current USCDI data element is articulated by the example measures included in “Disability Status,” which include the American Community Survey six-question set (ACS-6), Veterans RAND Health Survey (VR-12), and Patient-Reported Outcomes Measurement Information System (PROMIS) as equivalent examples under a single data element.[1] The ACS six-question set is defined as a demographic self-report instrument developed by a federal interagency committee for population-level identification—the same category of data collection as the race, ethnicity, sex, and primary language standards established under the same statute.[2,3] The VR-12 and PROMIS are clinical health assessment instruments that measures functioning and health-related quality of life to inform clinical decision-making. Compared to the ACS-6, the VR-12 and PROMIS instruments serve a fundamentally different purpose, are collected by different actors, at different points in the health journey of people with disabilities, and under different legal authorities.
Given the fundamental differences between collecting information about a population for service and accommodation access vs. about an individual patient to inform clinical decisions, we are requesting a new “Disability Status” data element under the Patient Demographics/Information data class to clearly separate out legally required demographic data from health assessment data.
[1] Draft USCDI V7 Disability Status data element and Accommodation data element, ASTP/ONC (healthit.gov).
[2] ACA Section 4302 (2010).
[3] U.S. Department of Health and Human Services Implementation Guidance on Data Collection Standards for Race, Ethnicity, Sex, Primary Language, and Disability Status. ASPE, Office of Health Policy (October 2011).
Use Case Description(s)
Use Case Description
Disability status data, as measured via population-level demographic data, is required for several federal efforts. The Affordable Care Act requires under Section 4302 the collection of disability status data as part of standardized population-level demographic data collection.[7] It is collected along with other demographic data, such as race, to inform population health work.
To align with this requirement, the Enhancing Oncology Model (EOM) requires, as of July 2024, collection of six well-tested disability questions that have been endorsed by the Office of the Assistant Secretary for Planning and Evaluation and the CDC, among others, as part of a CMS Innovation Center initiative to advance the collection of disability status data. These six questions have been used as part of the American Community Survey and many federal government surveys over the years.[7] Given this question set has been widely used and tested, EOM is requiring the collection and reporting of disability status as a population-level demographic via their sociodemographic data elements (SDEs) [8,9]:
“Disability status is a patient-reported demographic characteristic. Documentation of SDEs is necessary for providing high-quality. For some people with disabilities, their disability is a part of their identity and may affect how others perceive or interact with them, making it valuable to collect this information” (p. 6).[10]
Estimate the breadth of applicability of the use case(s) for this data element
The Enhancing Oncology Model (EOM) is a nationwide, episode-based payment model covering Medicare fee-for-service beneficiaries. At launch in 2023, the program included 44 oncology physician group practices encompassing 561 sites of care and more than 2,800 unique practitioners across approximately 37 states, with 3 commercial payer participants.
The DEC is a community of healthcare systems, clinicians, researchers, and others who are working to improve implementation of evidence-based, accessible healthcare for patients with disabilities. DEC hosts a national collaborative of 50+ health systems who are all working on disability accessibility initiatives. Most of the health systems are collecting or are in the planning stages of collecting patient disability status as a demographic in their electronic health records (EHRs). Health systems report collecting disability status to (1) identify and prepare for patients in need of accommodations; and (2) track health outcomes and improve the quality of care provided to patients with disabilities.
(1) In a published qualitative study, Dr. Megan Morris, Founder and Director of DEC, and her research team interviewed 17 participants representing 15 healthcare organizations (HCOs) that had active initiatives to implement systematic collection of disability status in the EHR. The study found that healthcare organizations reported their main purpose for collecting disability status was to prepare for patients with disabilities and their accommodation needs.[11] Not only does this information facilitate patients’ access to care, but it enables HCOs to better comply the Americans with Disabilities Act and other federal laws mandating they provide disability accommodations to patients when requested.
(2) Dr. Morris is currently leading an NIH-funded project (R01DC020188) to support primary care clinics at five health systems across the United States with the implementation of documenting patient’s communication disabilities in the EHR and provide necessary disability communication accommodations. All of the sites have developed EHR builds in which disability is collected and displayed in the patient’s demographics section of the chart.
(3) NYU Langone Health, where DEC is based, has used patient disability status as a demographic characteristic for quality improvement initiatives. For example, in 2025, NYU-affiliated Federally Qualified Health Centers found that patients who were deaf and used American Sign Language (ASL) scored lower on patient satisfaction scores. As a result, system leadership facilitated a focus group to understand these patients’ experiences. Patients shared obstacles they faced when accessing care, including limited availability of in-person interpreters, technology issues with video remote interpreting, inaccessible scheduling options, inaccessible after-visit summaries, and more. Using this information, system leadership developed a quality improvement plan to improve the experiences and quality of care delivered to their deaf patients.
[11] Morris MA, Sarmiento C, Eberle K. Documentation of Disability Status and Accommodation Needs in the Electronic Health Record: A Qualitative Study of Health Care Organizations Current Practices. Jt Comm J Qual Patient Saf. 2024;50(1):16-23. doi:10.1016/j.jcjq.2023.10.006
Estimate the breadth of applicability of the use case(s) for this data element
The Disability Status data element under the Patient Demographics/Information data class will apply across all healthcare settings and patient interactions with HCOs, from scheduling to after-visit summaries. Collecting patient disability status along with other demographic information they already collect allows HCOs to ensure that they are providing the same quality of care to all of their patients.
Mitigate health and health care inequities and disparities
Address the needs of underserved communities
Address public health interoperability needs of reporting, investigation, and emergency response
Maturity of Use and Technical Specifications for Data Element
Applicable Standard(s)
LOINC (recommended required fields): https://loinc.org/69919-9
LOINC Panel 69919-9, “Race, ethnicity, sex, primary language, disability - Health and Human Services (HHS) panel [HHS.ACA Section 4302]”, which includes the ACS six-question set.
LOINC (recommended optional fields): https://loinc.org/98067-2
LOINC Panel 98067-2, “Patient-centered disability questionnaire”, which questions comparable to the WG-SS on functioning plus optional question related to communication disabilities as well as the need for accommodations. https://loinc.org/69919-9
Additional Specifications
US Core 8.0.1 IG: https://hl7.org/fhir/us/core/STU8.0.1/screening-and-assessments.html
The US Core 8.0.1 IG includes the needed standard for the ACS through a value set in VSAC. Though this is currently under the disability related data element under Health Status Assessment, it still provides the standard to enable this new data element as it is untangled from the existing one.
The VSAC Disability Status Assessment value set (OID: 2.16.840.1.113762.1.4.1099.49) provides the ACS six-questions with a direct linkage to the LOINC codes in the LOINC Panel 69919-9, “Race, ethnicity, sex, primary language, disability - Health and Human Services (HHS) panel [HHS.ACA Section 4302]”. Specifically:
• 69856-3; Are you deaf, or do you have serious difficulty hearing?
• 69857-1; Are you blind, or do you have serious difficulty seeing, even when wearing glasses?
• 69858-9; Because of a physical, mental, or emotional condition, do you have serious difficulty concentrating, remembering, or making decisions?
• 69859-7; Do you have serious difficulty walking or climbing stairs?
• 69860-5; Do you have difficulty dressing or bathing?
• 69861-3; Because of a physical, mental, or emotional condition, do you have difficulty doing errands alone such as visiting a physician's office or shopping?
Current Use
(Level 2) Captured, stored, or accessed in multiple production EHRs or other HIT modules from more than one developer
Extent of exchange
(Level 2) Between more than two production EHRs or other HIT modules using available interoperability standards
Supporting Artifacts
The CMS Enhancing Oncology Model (EOM) requires collection of disability status using the ACS six-question set in production EHR environments across participating oncology practices starting in Performance Period 3 (July 2024). The list of participating health systems includes Texas Oncology with over 160 locations alone. In addition, both Massachusetts General Brigham and Kaiser Permanente use custom forms to capture this data and provide it to external entities to support a variety of needs, such as post-acute care transitions, regulatory reporting, and others via Health Information Exchanges. Cumulatively, exchange is occurring between multiple production EHR systems plus federal agencies through established reporting infrastructure. https://www.cms.gov/priorities/innovation/media/document/eom-sociodem-data-elem-guide
Potential Challenges
Restrictions on Standardization (e.g. proprietary code)
This data element is recommended to use LOINC (an open, freely available standard), specifically the ACS six-question set (LOINC Panel 69919-9). The primary standardization challenge is not proprietary codes but rather the current USCDI structure, which conflates two conceptually distinct domains—demographic self-report and clinical health assessment—under a single data element. This submission seeks to resolve that structural issue by establishing a separate demographic data element with clear terminology and purpose.
Restrictions on Use (e.g. licensing, user fees)
None known. LOINC codes are freely available under the Regenstrief Institute's open license. The ACS question set was developed by a federal interagency committee for public use in population surveys and carries no licensing or user fee restrictions.
Privacy and Security Concerns
Disability status as a self-reported demographic is protected health information (PHI) under HIPAA and subject to standard HIPAA privacy and security protections. Within those boundaries, this data can and should be shared across administrative staff (for appointment setup, coordination, and reasonable accommodation planning) and the healthcare team (to ensure accommodations are in place during clinical encounters). Notably, under ADA, Section 504, and ACA Section 1557, organizations have affirmative obligations to use this data to provide reasonable accommodations—including for caregivers with disabilities such as legal guardians and conservators. Self-reported disability status as a demographic characteristic does not invoke the heightened protections of 42 CFR Part 2 (substance use disorder records) or other specialized privacy frameworks. The data should be handled with the same privacy protections afforded to other demographic data elements such as race, ethnicity, sex, and primary language.
Estimate of Overall Burden
Implementation burden is low to moderate. The data element relies on patient self-reporting via a standardized six-question set already in widespread use across federal surveys such as the American Community Survey (Census), National Health Interview Survey (CDC), Current Population Survey (Labor Statistics). It does not require clinical calculation, specialized equipment, or external system integration. Collection can be integrated into existing patient intake and registration workflows alongside other demographic data (race, ethnicity, sex, primary language). EOM-participating practices have demonstrated that collection is feasible within standard EHR registration workflows with Epic being the largest vendor to meet this requirement. In addition, major EHR vendors (Epic, Oracle Health) already support custom form creation sufficient to capture these questions. The primary implementation effort involves configuring intake forms and ensuring the data maps to the correct LOINC codes, which is a routine EHR configuration task rather than a significant development effort.
Other Implementation Challenges
Adoption and workflow challenges include: (1) Training registration and intake staff to ensure collection of disability status occurs consistently and sensitively alongside other demographic data, as this represents a newer addition to demographic collection compared to race, ethnicity, and sex. (2) Ensuring patients understand the purpose of the questions as demographic data collection for health surveillance purposes rather than clinical assessment, which requires careful framing of the questions during intake. (3) Addressing the current structural conflation in USCDI, where demographic self-report and clinical health assessment instruments are grouped under a single data element—this may cause confusion among implementers about which instruments to use and for what purpose. Resolving this conflation through the requested data element separation would reduce, rather than increase, implementation burden by providing clear guidance on the distinct purposes and workflows for each domain.
ASHA is the national professional, scientific, and credentialing association for 247,000 members, certificate holders, and affiliates who are audiologists; speech-language pathologists (SLPs); speech, language, and hearing scientists; audiology and speech-language pathology assistants; and students. Audiologists specialize in preventing and assessing hearing and balance disorders as well as providing audiologic treatment, including hearing aids. SLPs identify, assess, and treat speech, language, swallowing, and cognitive communication disorders. The American Speech-Language-Hearing Association (ASHA), supports the PACIO Project recommendations to the Office of the National Coordinator for Health Information Technology (ONC) to:
Rename the existing "Disability Status" data element under the Health Status Assessments data class to "Disability Assessment" and provide a refined definition and updated examples for the data element.
Add a Disability Status data element under the Patient Demographics/Information data class, consistent with the HHS Data Council’s own Implementation Guidance and with the intent of Section 4302 of the Affordable Care Act (ACA).
Together, these recommendations address a critical issue in the current structure, which conflates clinician-documented evaluation with patient-reported information and identity, including communication-related disability and access needs, contributing to inconsistency in documentation and its use.
Renaming the existing element to “Disability Assessment” more accurately reflects its function as a clinical evaluation of health status and supports more consistent and appropriate use within care planning and documentation workflows. This is particularly relevant for people with communication-related disabilities, where clinical assessment informs care planning but does not replace patient-reported needs related to communication access. This distinction is necessary for maintaining data integrity and ensuring that assessment data do not serve as proxy for patient-reported demographic information.
Placement of Disability Status within Demographics is necessary to ensure consistent, longitudinal data capture across encounters, providers, and health systems. In contrast to assessment data, which are often episodic and context-dependent, demographic data elements are more reliably exchanged through interoperable systems, including consistent identification of communication access needs across care settings. They are better positioned to support care coordination, population health measurement, and quality reporting.
In addition, aligning Disability Status with the corresponding Accommodations data element within the Demographics data class enhances the operational utility of the data. Structuring both elements at the demographic level enables standardized identification and transmission of accommodation needs across workflows, including intake, triage, and care delivery, and supports implementation through clinical decision support tools, flags, and other health IT functionalities. This is particularly important for people with communication disorders and differences, where timely access to appropriate supports is foundational to safe and effective care.
Collectively, these updates will facilitate more reliable data exchange, reduce variability in documentation practices, and enable more robust analysis of disparities in access, care process, and outcomes for people with disabilities. These changes represent advancements in interoperability, continuity of care, and patient-centered health care delivery.
The Disability Equity Collaborative (DEC) is a community of engaged stakeholders — including disability advocates, researchers, healthcare organizations, and others committed to improving disability access in healthcare. We write today to urge the Office of the National Coordinator for Health Information Technology (ONC) to adopt the recommendations of the PACIO Project, which we believe are essential to ensuring that disability data is captured accurately and meaningfully within the United States Core Data for Interoperability (USCDI):
Rename the existing "Disability Status" data element under the Health Status Assessments data class to "Disability Assessment," accompanied by a refined definition and updated examples.
Add a new Disability Status data element under the Patient Demographics/Information data class, consistent with the HHS Data Council's own Implementation Guidance and with the intent of Section 4302 of the Affordable Care Act (ACA).
We cannot overstate the importance of this distinction. As it stands, the current structure conflates two fundamentally different concepts — and the consequences for people with disabilities are real.
Disability Status is not assessed — it is a patient-reported demographic. Disability Status questionnaires, like the American Community Survey (ACS) questions, are survey instruments designed to identify people with disabilities. In the healthcare setting, this information serves critical purposes: it drives quality improvement efforts and determines whether a patient is entitled to reasonable accommodations under the Americans with Disabilities Act. These questions are not typically administered by clinicians and are not used to evaluate functioning. They belong where all demographic data belongs — under Patient Demographics/Information.
Disability Assessment, by contrast, refers to clinician-administered evaluations using validated health assessment tools such as the VR-12 and PROMIS. These instruments measure health outcomes across multiple domains that contribute to a person's quality of life. They evaluate a patient's functioning and impairment and are essential for providers developing treatment or care plans specifically related to that impairment.
We urge ASTP/ONC to recognize that disability status and clinical impairment are not interchangeable. A person's disability status is not necessarily reflective of their clinical diagnosis. As the International Classification of Functioning makes clear, disability is the intersection of a person's impairment and the external factors in their environment. Health assessment tools like the VR-12 and PROMIS measure impairment — they do not and cannot determine disability status. There is no reliable method to derive a patient's disability status from diagnostic codes or assessment instruments. It must be recorded as a patient-reported demographic.
Without this change, we risk perpetuating a data infrastructure that obscures the needs of people with disabilities rather than illuminating them. We respectfully but firmly call on ONC to act on these recommendations and ensure that USCDI reflects the lived reality of the disability community.
Sincerely,
Dr. Megan Morris
Founder and Director
Disability Equity Collaborative
Eve Schoenberg
Project Coordinator
Disability Equity Collaborative
Cedars-Sinai
Indira Shenoy
Director – Quality & Accessibility
Dana-Farber Cancer Institute
Sherri Rita
Director, Enterprise Regulatory Services, Civil Rights
Kaiser Permanente
Annika Agrawal
Director of Advocacy & Policy
Medical Students with Disability and Chronic Illness
Kara Ayers
Director
National Center for Dignity in Healthcare and Community Living for People with Disabilities
Doreen Bestolarides, RN
Family Advocacy and Policy Committee
AADMD
Holly Brown
Executive Director
Golisano Institute for Developmental Disability Nursing
David A Ervin
CEO
Makom
Anjali Forber-Pratt
Director of Research
American Association on Health & Disability
Emily Johnson
VP Policy and Advocacy
American Academy of Developmental Medicine and Dentistry
Seth M Keller
Co-President
National Task Group on Intellectual Disabilities and Dementia Practices
Phillip Mason
Executive Director
CCHS Network
John J. Mulholland, Jr., Esq., CAE
Executive Director
New Jersey Association of Special Education Partner Schools
Rick Rader, MD
Editor in Chief
HELEN, The Journal of Human Exceptionality
Clarke Ross
Lakeshore Foundation Washington Representative
Lakeshore Foundation
Vanessa Rastović
Advocacy, Sr. Director
Project DIME
Carole Schwartz
President
Alliance for Disability in Health Care Education
Neil Snyder
Director of Public Policy
Hearing Loss Association of America
Bonnielin Swenor
Director
Johns Hopkins Disability Health Research Center
Albright Alitsi
Tami Altschuler
Zary Amirhosseini
Disability Program Manager
Nicole Bohn
Camylle Boxton
Marie Coppola
Jennifer Duffecy
Peggy Ellertsen
Rachel Cometa Estuar
Operations Manager
Brooke Cruz
Jody Greenhalgh
Occupational Therapist - Tertiary Medical Center + Disability, Health, Accessibility Safety Officer
Lilly Grossman
Thomas Haber
Jean P. Hall
Research Professor Emerita
Toni Iacolucci
Co-Creator, Healthcare with Hearing Loss
Communication Access in Healthcare – HLAA
Patricia Islas
Rebecca Kronk
Liz Long
PJ Lutz
Della Mahoney
UC Law San Francisco
Marilee McGraw, RN
Shirley McMillan
consuli
Lisa Meeks
Austin Nugent
Jennifer Oshita
Grayson Schultz
Sara Shunkwiler
Martha L. Simmons, MD
Xigrid Soto-Boykin
Researcher; Policy Analyst
Mahsa Tahzibi
Dennis Tran
Abidin Hakan Tuncer
Karen Turner
Autism and Developmental Disability Clinical Case Manager
Independent capture of Disability Status as a Patient Demographic in the United States Core Data for Interoperability (USCDI), separated from rather than included along with disability assessments, is a foundational step toward equal health treatment for the more than one in four American adults who report living with a disability. Based on the consensus of the PACIO Disability Status Work Group — comprising clinicians, EHR vendors, health systems, disability advocates, and federal agency participants — the PACIO Community respectfully urges the Assistant Secretary for Technology Policy (ASTP) to:
Rename the existing "Disability Status" data element under the Health Status Assessments data class to "Disability Assessment" and provide a refined definition and updated examples for the data element.
Add a Disability Status data element under the Patient Demographics/Information data class, consistent with the HHS Data Council’s own Implementation Guidance and with the intent of Section 4302 of the Affordable Care Act (ACA). A corresponding ONDEC submission is forthcoming.
These recommendations aim to disambiguate between demographic and clinical uses of disability-related data by clarifying that (1) the Health Status Assessments element captures clinician-collected health assessment data and (2) the new Patient Demographics/Information element captures self-reported disability status as a demographic characteristic.
The attachment to this comment documents the benefits that proper capture of “Disability Status” as a demographic will enable: closing persistent gaps in health surveillance, unlocking cross-system interoperability for demographics across federal agencies and post-acute care settings, reducing conflation of demographics with clinical assessment, and advancing patient autonomy. It also addresses the functional framing of the American Community Survey six-question set (ACS-6) on disability and demonstrates that this framing is immaterial to its classification as a demographic data element.
For the complete rationale, three-domain framework synopsis, and supporting references, please see the attached document.
The American Association on Health and Disability and the Lakeshore Foundation appreciate the opportunity to provide comments to the Office of the National Coordinator for Health Information Technology.
The American Association on Health & Disability (AAHD) is a national nonprofit organization (www.aahd.us) committed to advancing health equity, community inclusion, and wellness for people with disabilities through research, policy, and knowledge translation. AAHD is focused on addressing systemic barriers to health inequity, strengthening disability data infrastructure, and advancing a human rights–based approach to disability across research and healthcare systems. The Lakeshore Foundation (www.lakeshore.org) mission is to enable people with physical disability and chronic health conditions to lead healthy, active, and independent lifestyles through physical activity, sport, recreation and research. Lakeshore is a U.S. Olympic and Paralympic Training Site; the UAB/Lakeshore Research Collaborative is a world-class research program in physical activity, health promotion and disability linking Lakeshore’s programs with the University of Alabama, Birmingham’s research expertise.
We appreciate the opportunity to provide comment and strongly urge the Assistant Secretary for Technology Policy/Office of the National Coordinator for Health Information Technology (ASTP/ONC) to adopt the recommendations of the PACIO Project to improve the representation of disability within the United States Core Data for Interoperability (USCDI).
Specifically, AAHD supports the following actions:
Renaming the existing “Disability Status” data element under the Health Status Assessments data class to “Disability Assessment,” with a clarified definition and updated examples.
Adding a new “Disability Status” data element under the Patient Demographics/Information data class, consistent with the HHS Data Council’s Implementation Guidance and the intent of Section 4302 of the Affordable Care Act.
AAHD strongly urges ASTP/ONC to adopt the recommendations of the PACIO Project that include making this important distinction. This distinction is foundational to the disability community and from our organizational commitment to improving the quality, equity, and utility of disability data and ensuring that data systems accurately reflect the lived experiences of people with disabilities. Improving the quality and consistency of disability data is essential to delivering equitable healthcare, particularly in light of the well-documented disparities experienced by people with disabilities across healthcare access, quality, and outcomes. When healthcare systems systematically collect and use accurate disability data, they are better equipped to identify unmet needs, tailor care, allocate resources effectively, and monitor progress toward reducing these disparities.
Disability status is a patient-reported demographic characteristic, not a clinical determination. The Federal Evidence Agenda on Disability clearly states, “Physical examinations are never appropriate for identity documentation.” (p. 43, 2025). Additionally, research shows that disability self-identification remains notably misaligned with the prevalence of health conditions, reflecting a gap shaped by a range of social, cultural, and structural factors that are well-studied and understood by the disability community (i.e., Bogart et al., 2017; Hall et al., 2022). Meaning, even with the presence of health conditions, many individuals do not report disability on their own. Additionally, asking individuals to self-report disability identification is different than asking individuals to self-report functional limitations—which is what the widely used American Community Survey (ACS) 6 questions do. Many use measures such as the ACS-6 as a proxy for self-reported disability, however, researchers are working to explore better ways of asking those questions since functional limitations are not always the same as how much a disability is a part of a person's identity (See Landes et al, 2025). Until the measurement science catches up, however, the widely adopted ACS-6 questions would provide a helpful and unique data element under the patient demographics/information data class.
The combination of self-reported functional limitations from patient demographics AND clinical assessment of disability from clinicians gives a more complete picture of individuals with disabilities. Clinical diagnoses identify specific medical conditions based on standardized criteria, while self-report about functional limitations reflects how individuals experience functional limitations and participation in daily life—often shaped by social and environmental barriers that clinical measures may miss. Because disability is both a medical and lived, contextual experience, relying on only one approach provides an incomplete picture. We need both to ensure accurate data, equitable policy, and research that truly reflects the realities of disabled people’s lives. It should be noted that self-reported disability identity status is a different type of question that is not currently reflected in the proposed changes.
In reality, there may be alignment between both clinical assessment and self-report of functional limitations, as these individuals have a documented condition and also acknowledge the limitations presented because of that disability and may embrace disability as part of their identity. Though, there may also be examples from the disability community and supported by research that shows misalignment: For example, individuals may meet the criteria of disability based on clinical assessment but do not self-report functional limitations. This could be due to stigma, cultural factors, using assistive devices that minimize the impacts on functional limitations, age—late onset or individuals aging into disability are less likely to self-report functional limitations. There may also be individuals who self-report functional limitations but do not have a clinical assessment that corroborates, this often occurs for hard to diagnose conditions, as one example, or fluctuating conditions that make clinical assessment at a specific moment in time challenging, yet these individuals may experience functional limitations, chronic conditions, or disabling environments even in the absence of a formal diagnosis.
As such, if policy relies only on clinical diagnosis, it may miss people who are functionally impacted or are undiagnosed. If it relies only on self-reported functional limitations, it may miss those who qualify clinically but based on their environmental set up or assistive devices used they may not report functional limitations, as an example. Using both approaches helps create a more complete understanding of disability across populations. Therefore, we urge ASTP/ONC to recognize that disability status and clinical impairment are not interchangeable and that there is a need to better develop strategies for capturing data during clinical encounters to improve healthcare delivery that addresses the unique and evolving needs of people with and without disabilities.
Thank you for the opportunity to comment. If you have any questions please contact Anjali Forber-Pratt at aforberpratt@aahd.us
Submitted byMegan Morris on
The following are comments from multiple health systems representatives within the Disability Equity Collaborative's Leaders Learning Collaborative:
1. Disability status as a demographic and associated accommodations data needs to be captured
“Capturing disability status—as a demographic—and linked accommodations data is essential for providing equitable, person-centered care. Disability is a protected class under federal nondiscrimination laws (ADA, Section 504, HHS Section 1557 Final Rule). Without systematically capturing this information, organizations cannot identify disparities, ensure accessibility, proactively meet accommodation needs, or comply with legal and regulatory mandates.”
“Capturing disability as a demographic ensures that it is respected and treated with the same importance, and permanence, as age, sex, race, language, etc. It enables quick, convenient, and universal visibility across care providers: registration, scheduling, transfer, patient experience, etc. No one has to “dig in the chart” to find this information. It supports timely delivery of aids and services when coupled with the appropriate accommodation need (e.g., deaf with ASL interpreter; blind with qualified readers, etc.).
“Treating [disability status] as a demographic helps us understand our patient population and address equity gaps…We can’t assume these needs based on diagnoses.”
“Having a standardized method for capturing disability status and accommodation needs supports clinicians and the broader care team—particularly support staff who frequently communicate essential information to patients. Standardized documentation ensures that disability-related needs are consistently recognized, respected, and integrated into every stage of the care experience.”
Example
“A patient who is Deaf and uses ASL marks “Deaf/Hard of Hearing” in their demographic disability field and selects “ASL interpreter” under accommodations. This information automatically flows to scheduling, the visit record, and interpreter services, ensuring an ASL interpreter is booked before every appointment, preventing last-minute scrambling and ensuring legal compliance.”
2. How disability status is currently or is planned to be used:
Clinical Care: Alerts clinicians and care teams so they can prepare accessible equipment (e.g., height-adjustable exam table), communication tools (e.g., interpreter, communication board), and care modifications.
Operational Planning: Helps organizations forecast demand for accessible equipment, sensory-friendly environments, or specific communication supports.
Quality & Safety: Allows monitoring of missed appointments, long wait times, or adverse events among patients with disabilities to identify disparities.
Digital Accessibility: Ensures patient portal, telehealth, and digital communications are usable for those with screen readers, cognitive needs, or low vision.
Research & Equity Analytics: Supports disability-inclusive research design
Emergency Preparedness: Enables identification of patients needing assistance during evacuation or emergency communications.
Human Resources & Workforce Inclusion: When used for employees, supports accommodation planning, workspace accessibility, and trend analysis.”
“Demographic data, including disability status and accommodation needs, is routinely shared with an individual’s health plan, specialty providers, and partnering services such as home health and rehabilitation. Ensuring that all participating providers and organizations have access to this critical information strengthens care coordination, supports continuity, and enables timely planning for appropriate accommodations. Ultimately, this improves the safety, accessibility, and effectiveness of the care delivered across settings.”
“We use this data to make sure the right supports are in place before a visit and throughout a patient’s care. This includes scheduling, communication preferences, equipment needs, care-team awareness, and coordinating services like interpreters. It also helps with broader work—quality improvement, health equity efforts, and planning for resources across the system.”
Example
“After collecting disability demographic data, the Quality & Safety office finds that patients with mobility disabilities experience lower rates of cancer screening due to inaccessible equipment. This triggers a systemwide initiative to purchase height-adjustable tables and wheelchair-accessible mammography equipment.”
3. What needs are satisfied if/when your organization documents this information
A. Patient Needs-Ensures care is accessible, safe, and respectful. Reduces the burden on patients to repeatedly explain their disability or accommodation requirements. Improves satisfaction, trust, and overall patient experience. Enables proactive planning (e.g., longer appointment times, accessible transport instructions).
B. Provider & Staff Needs-Reduces uncertainty by providing clear information before the visit. Improves efficiency by avoiding last-minute problem-solving. Enhances staff confidence in delivering equitable, compliant care.
C. Organizational Needs-Supports compliance with ADA, Section 504, HHS Final Rule, Joint Commission, and CMS requirements. Enables systemwide reporting and performance improvement. Strengthens readiness for legal audits or disability-related complaints. Demonstrates commitment to health equity and inclusive care.
D. Systemwide Equity & Research Needs-Ensures people with disabilities are included in research in ethical, accessible ways.”
“This information allows us to understand the specific needs of the patient population we serve and the accommodations necessary for patients to fully access care. It can also be used to guide targeted disability-competency training for clinicians and support staff—training that is essential for building clinical confidence and addressing the negative behaviors or attitudes that patients with disabilities too often encounter…”
“…from a system standpoint, it allows us to track outcomes, understand disparities, and make sure accommodations follow patients across settings so they don’t have to repeat their needs over and over.”
“Documenting disability status and related accommodation needs allows healthcare organizations to deliver the right aid to the right person at the right time; provide history of patient needs and preferences (VRI vs. in person interpretation, etc.); anticipate and prepare for the needs of repeat patients; collect data for quality improvement initiatives; and ensure consistency and reliability across the healthcare system (doctor clinic, hospital, imaging center, etc.)”
Disability Rights Education and Defense Fund (DREDF) is a national cross-disability law and policy center that protects and advances the civil and human rights of people with disabilities through legal advocacy, training, education, and development of legislation and public policy. We are committed to increasing accessible and equally effective healthcare and opportunities for people with disabilities so they can lead full, productive lives in the communities of their choice.
We submit this comment to strongly support recommendations made by the Post-Acute Care InterOperability (PACIO) Project to reclassify Disability Status from its current classification under the US Core Data for Interoperability (USCDI) as an element of Health Status Assessments to classification as an element of Demographic Identification. In doing so, we are not claiming that disability status is irrelevant for health status. Rather, we assert that disability status is far more relevant to demographic and social identity, in the same way that race/ethnicity, gender, income, and other personal characteristics are recognized as demographic elements. The functional disability questions for disability status do not have a one-to-one relationship with precise clinical measurements, and they also cannot be directly mapped onto binary models such as healthy/unhealthy or well/unwell. Rather, the true value of the disability status questions lies in how they enable people with disabilities to recognize themselves and thereby count as subjects of needed research, individual patients who need accommodations and policy modifications to receive effective healthcare, and persons who experience multiple health-related barriers.
Granular research that will further unearth ongoing health inequities that are not attributable to clinical explanation, and that will aid law and policy makers to address the barriers and gaps in education, knowledge, and systems that lie behind disability-related healthcare disparities
Disability identification that will trigger data and IT systems to obtain information needed for an accommodations data element that could finally enable people with various disabilities to receive equally effective healthcare;
Research that can examine how disability interacts with other demographic factors and within/among subpopulations, allowing us to gain a fuller understanding of individuals can experience compounded barriers to health and healthcare
For similar reasons, we also strongly endorse the advancement of the Accommodation data element to at least Level 2, as recommended by Centers for Disease Control (CDC) and the Centers for Medicare and Medicaid - Center for Clinical Standards and Quality (CMS-CCSQ) in their submitted comments.
As identified in many of the comments submitted in support of the PACIO Disability Status and Accommodations recommendations, the disability community is finally seeing movement in the healthcare system to acknowledging disability status as a demographic element. Electronic health record vendors such as EPIC Systems are finally recognizing how health record keeping affects people with disabilities, health plans and clinics are developing ways to keep and use accommodations data, there are efforts at state and county levels to accurately gather demographic disability data. USCDI should be at the forefront of these efforts, helping to ensure consistency of, and guidance on, necessary disability data characterization.
As an organization is run by and for people with disabilities, DREDF calls for the adoption of the PACIO recommendations as a step that will help further advance the federal demographic data collection standards implemented by the federal Department of Health and Human Services almost 14 years ago.
Submitted by Silvia Yee, Policy Director, Disability Rights Education and Defense Fund (DREDF)
Disability Rights Education and Defense Fund (DREDF) is a national cross-disability law and policy center that protects and advances the civil and human rights of people with disabilities through legal advocacy, training, education, and development of legislation and public policy. We are committed to increasing accessible and equally effective healthcare and opportunities for people with disabilities so they can lead full, productive lives in the communities of their choice.
We submit this comment to strongly support recommendations made by the Post-Acute Care InterOperability (PACIO) Project to reclassify Disability Status from its current classification under the US Core Data for Interoperability (USCDI) as an element of Health Status Assessments to classification as an element of Demographic Identification. In doing so, we are not claiming that disability status is irrelevant for health status. Rather, we assert that disability status is far more relevant to demographic and social identity, in the same way that race/ethnicity, gender, income, and other personal characteristics are recognized as demographic elements. The functional disability questions for disability status do not have a one-to-one relationship with precise clinical measurements, and they also cannot be directly mapped onto binary models such as healthy/unhealthy or well/unwell. Rather, the true value of the disability status questions lies in how they enable people with disabilities to recognize themselves and thereby count as subjects of needed research, individual patients who need accommodations and policy modifications to receive effective healthcare, and persons who experience multiple health-related barriers.
Granular research that will further unearth ongoing health inequities that are not attributable to clinical explanation, and that will aid law and policy makers to address the barriers and gaps in education, knowledge, and systems that lie behind disability-related healthcare disparities
Disability identification that will trigger data and IT systems to obtain information needed for an accommodations data element that could finally enable people with various disabilities to receive equally effective healthcare;
Research that can examine how disability interacts with other demographic factors and within/among subpopulations, allowing us to gain a fuller understanding of individuals can experience compounded barriers to health and healthcare
For similar reasons, we also strongly endorse the advancement of the Accommodation data element to at least Level 2, as recommended by Centers for Disease Control (CDC) and the Centers for Medicare and Medicaid - Center for Clinical Standards and Quality (CMS-CCSQ) in their submitted comments. When people with disabilities are consistently asked about the healthcare accommodations and policy modifications that they need, and when that information is consistently recorded and used, we will be that much closer to achieving health, choice, and independence as individuals and as a community.
As identified in many of the comments submitted in support of the PACIO Disability Status and Accommodations recommendations, the disability community is finally seeing movement in the healthcare system to acknowledging disability status as a demographic element. Electronic health record vendors such as EPIC Systems are finally recognizing how health record keeping affects people with disabilities, health plans and clinics are developing ways to keep and use accommodations data, there are efforts at state and county levels to accurately gather demographic disability data. USCDI should be at the forefront of these efforts, helping to ensure consistency of, and guidance on, necessary disability data characterization.
As an organization is run by and for people with disabilities, DREDF calls for the adoption of the PACIO recommendations as a step that will help further advance the federal demographic data collection standards implemented by the federal Department of Health and Human Services almost 14 years ago.
As a disability/health scholar and social work professional who co-chairs the WHO Functioning and Disability Reference Group, I strongly support the recommendation to move disability status from Health Status Assessments to Patient Demographics.
The change would signify an important shift in health care where disability moves away from being viewed as an individual medical problem to a recognized aspect of identity shaped by societal factors. The shift better aligns with global standards and terminology reflected in the International Classification of Functioning, Disability and Health, or ICF, where disability refers to the interaction between a person's health condition(s) and their contextual factors (environmental and personal factors).
Collecting disability data in health records is a crucial first step toward identifying disparities in care and health outcomes that individuals with disabilities experience. It enables tracking differences in health statistics, such as disease prevalence and access to preventive services, between persons with and without disabilities.
Documenting disability status as a patient demographic will allow healthcare providers to better identify and provide necessary accommodations and auxiliary aids, such as sign language interpreters or adjustable exam tables, to ensure equitable and effective care.
This recommendation promotes a more inclusive approach to healthcare by allowing patients to report their own disability status, moving beyond a sole reliance on diagnostic codes often considered problematic.
Comments submitted by Barbara Kelley, Executive Director, Hearing Loss Association of America.
Disability is a demographic characteristic, not a clinical condition. Its current placement under Health Status Assessments risks conflating disability with illness or impairment, which can lead to misinterpretation and unintended consequences in care delivery and data analysis. Reclassifying Disability Status under Patient Demographics/Information would:
Align with federal guidance from the HHS Data Council and CMS practices.
Promote more accurate and respectful representation of individuals with disabilities.
Enhance the utility of demographic data for equity analysis, population health, and policy development.
This change is essential to ensure that disability data is treated with the same rigor and respect as other demographic elements such as race, ethnicity, and gender identity.
Recommendation: Recommend moving the Disability Status data element to the Patient Demographics/Information data class.
Rationale: The PACIO Project Community* recognizes and appreciates the significant work undertaken by the HHS Data Council in developing the Disability Status data collection standards. We understand the historical context and the deliberate efforts made by the Council and its dedicated workgroup to ensure that this data accurately captures necessary information, particularly as it relates to demographic data collection. The Council’s approach, as outlined in the "U.S. Department of Health And Human Services Implementation Guidance on Data Collection Standards for Race, Ethnicity, Sex, Primary Language, and Disability Status" clearly demonstrates that Disability Status is intended to be collected as part of demographic information, alongside race, ethnicity, and sex.
The PACIO Community’s ongoing concern is that Disability Status under USCDI continues to be classified under the Health Status Assessments data class, which does not reflect its primary purpose as a demographic identifier. Disability Status, like race, ethnicity, and sex, is a fundamental demographic characteristic and should be grouped accordingly to ensure consistency and clarity in data collection and use. Moving this data element to the Patient Demographics/Information data class would better align with the intent of the HHS Data Council and the standards described in the aforementioned guidance document.
Furthermore, collecting the patient asserted Disability Status as part of Health Status Assessments risks conflating disability with clinical health assessments, which may lead to misinterpretation or unintended consequences, such as influencing disability benefits or incorrectly classifying patients. Disability, as a demographic characteristic, does not inherently reflect a person’s health status, functional status, or cognitive status, which is typically captured under Health Status Assessments.
This recommendation is consistent with current practices in post-acute care (PAC) settings and aligns with CMS guidance, Inventory of Resources for Standardized Demographic and Language Data Collection. By classifying Disability Status within Patient Demographics/Information, we can more accurately capture and utilize this data for demographic analysis, support better clinical decision-making, and avoid conflating disability assertions with health assessments.
* The PACIO (Post-Acute Care Interoperability) Project, established February 2019, is a collaborative effort between industry, government, and other stakeholders, that aims to advance interoperable health information exchange between post-acute care (PAC) providers, patients, and other key stakeholders across health care.
The "Optional Background Text / Cover Letter" field provides space for additional context or introductory information related to your comment.
If you wish to provide context, explanation, or an introduction to your comment, enter this information in the field labeled "Optional Background Text / Cover Letter." This is entirely optional and is most useful when submitting multiple related comments or when additional background would help reviewers understand your feedback.
If you are only commenting on a single data class or element, you may leave this field blank.
2. Select the Data Class
To specify which data class your comment addresses:
In the "Data Class" drop-down menu, select the appropriate data class you want to comment on.
If you are providing a general comment that is not specific to a data element, select "General" from the options. Comments with this designation will be displayed on the USCDI landing page.
Note that the Data Class field will automatically populate based on your current location in the platform:
If you are on a data class page, the field will be set to that specific data class
If you are on a data element page, the corresponding data class will be pre-selected
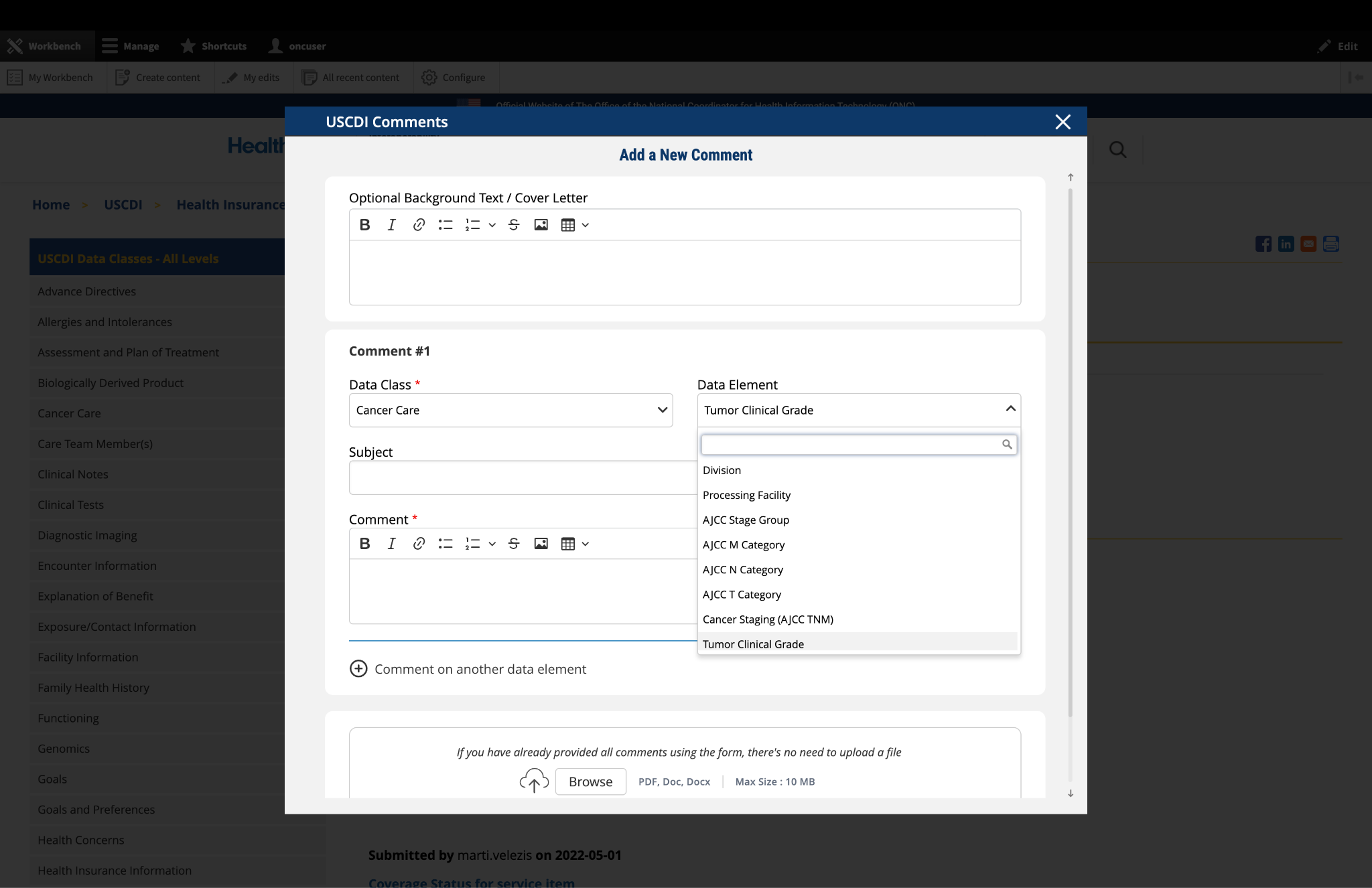
3. Select the Data Element
To specify which data element your comment addresses:
In the "Data Element" drop-down menu, select the specific data element you want to comment on.
The drop-down menu will display only the elements available under the data class you selected in the previous step.
You can use the search function within the drop-down to quickly locate a specific data element.
If you are commenting on the data class itself rather than a specific element, you may leave this field blank.
Note: Comments on a specific data element will appear on the respective data element page, while comments on a data class (without a specific element selected) will appear on the landing page for that data class.
Fig 1 The "Data Class" and "Data Element" dropdown menus allow users to specify the exact content they wish to comment on.
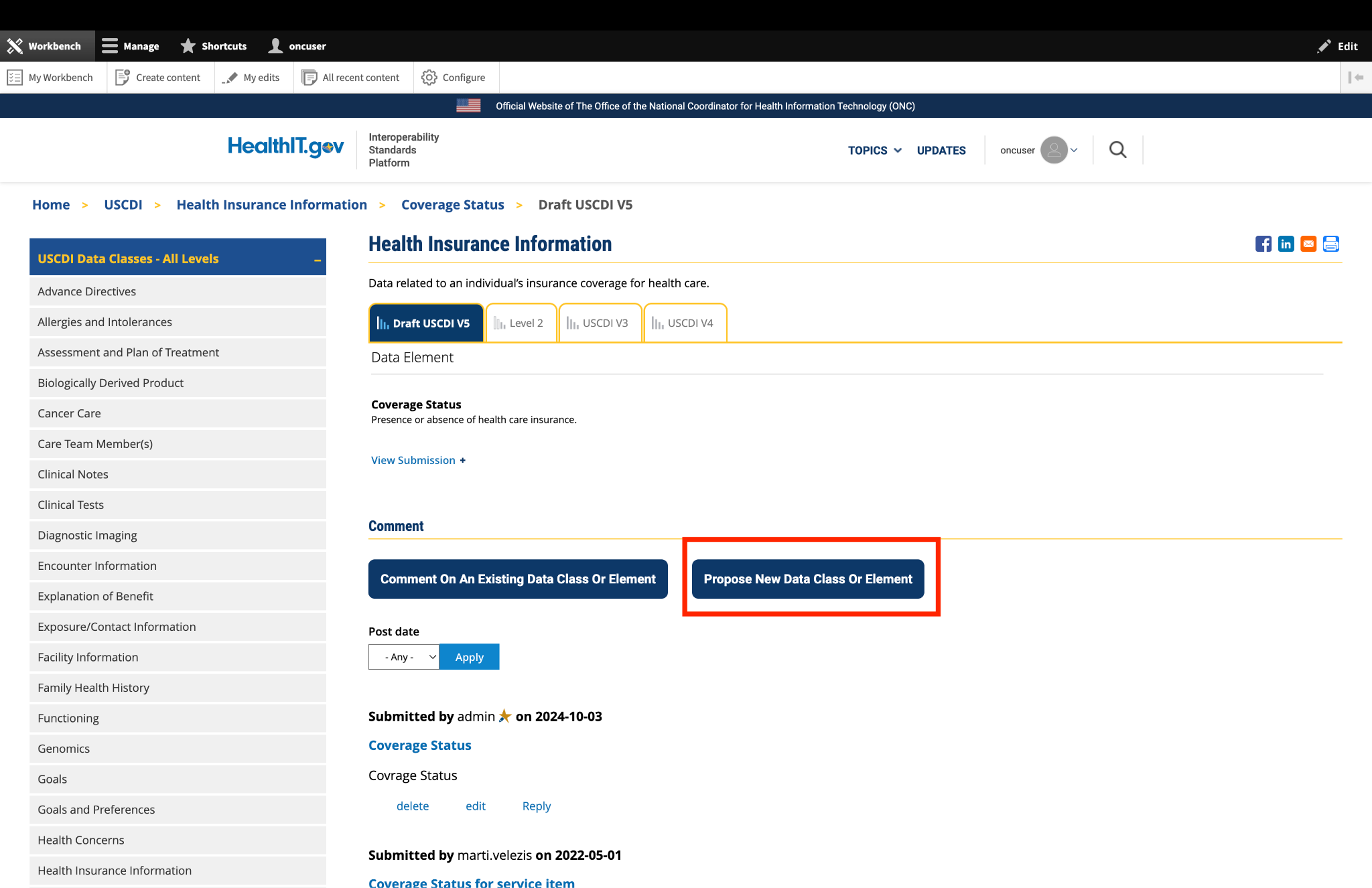
4. Optional: Propose New Data Class or Element
If you cannot find the appropriate data class or element for your comment:
Instead of clicking the "Comment On An Existing Data Class Or Element" button, click the adjacent button labeled "Propose a New Data Class or Data Element."
This will redirect you to the ONDEC (ONC New Data Element and Class) Submission System.
In the ONDEC system, follow the provided instructions to submit your proposal for a new data class or element.
Once your proposal is submitted through ONDEC, it will be reviewed separately from the commenting process.
Fig 2 The "Propose a New Data Class or Data Element" button redirects users to the ONDEC Submission System for proposing new data elements not currently available in the system.
5. Complete the Comment Form
Fill out the required fields in the comment form:
Subject: Enter a brief, descriptive title that summarizes your comment. This helps reviewers quickly understand the nature of your feedback.
Comment: In this field, provide the full details of your comment or feedback. Be as clear and specific as possible about your suggestions, concerns, or observations. Include any relevant details that support your position.
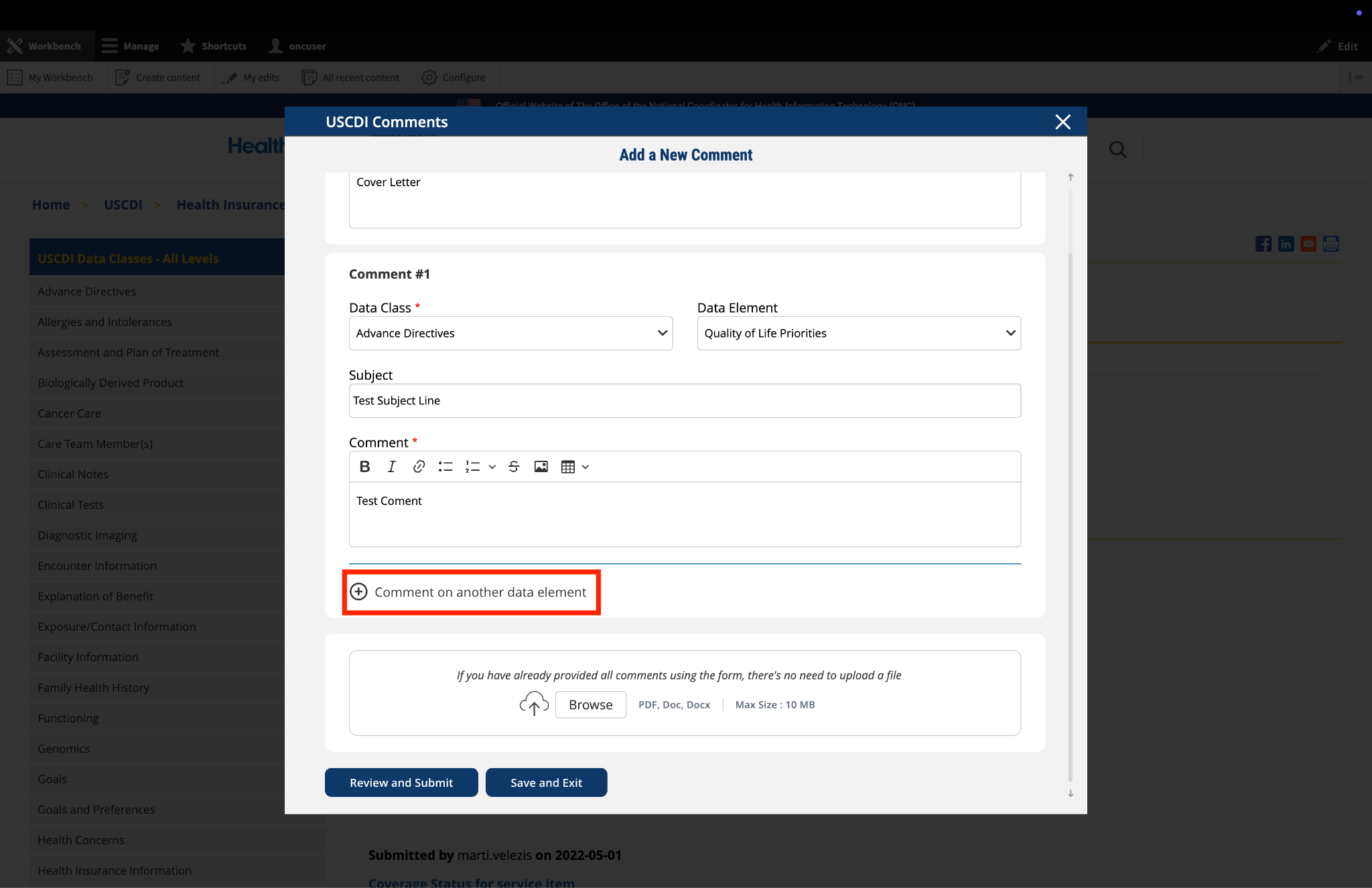
6. Optional: Add Additional Comments
If you need to comment on multiple data classes or elements:
After completing your first comment, click the link labeled "Comment on another data element" at the bottom of the form.
A new comment section will appear, allowing you to enter details for your additional comment.
For each additional comment, you must select the appropriate data class and data element from the drop-down menus.
Complete the Subject and Comment fields for your additional comment.
Repeat this process for each additional comment you wish to submit.
Fig 3 The "Comment on another data element" link enables users to create multiple comments addressing different elements within a single submission.
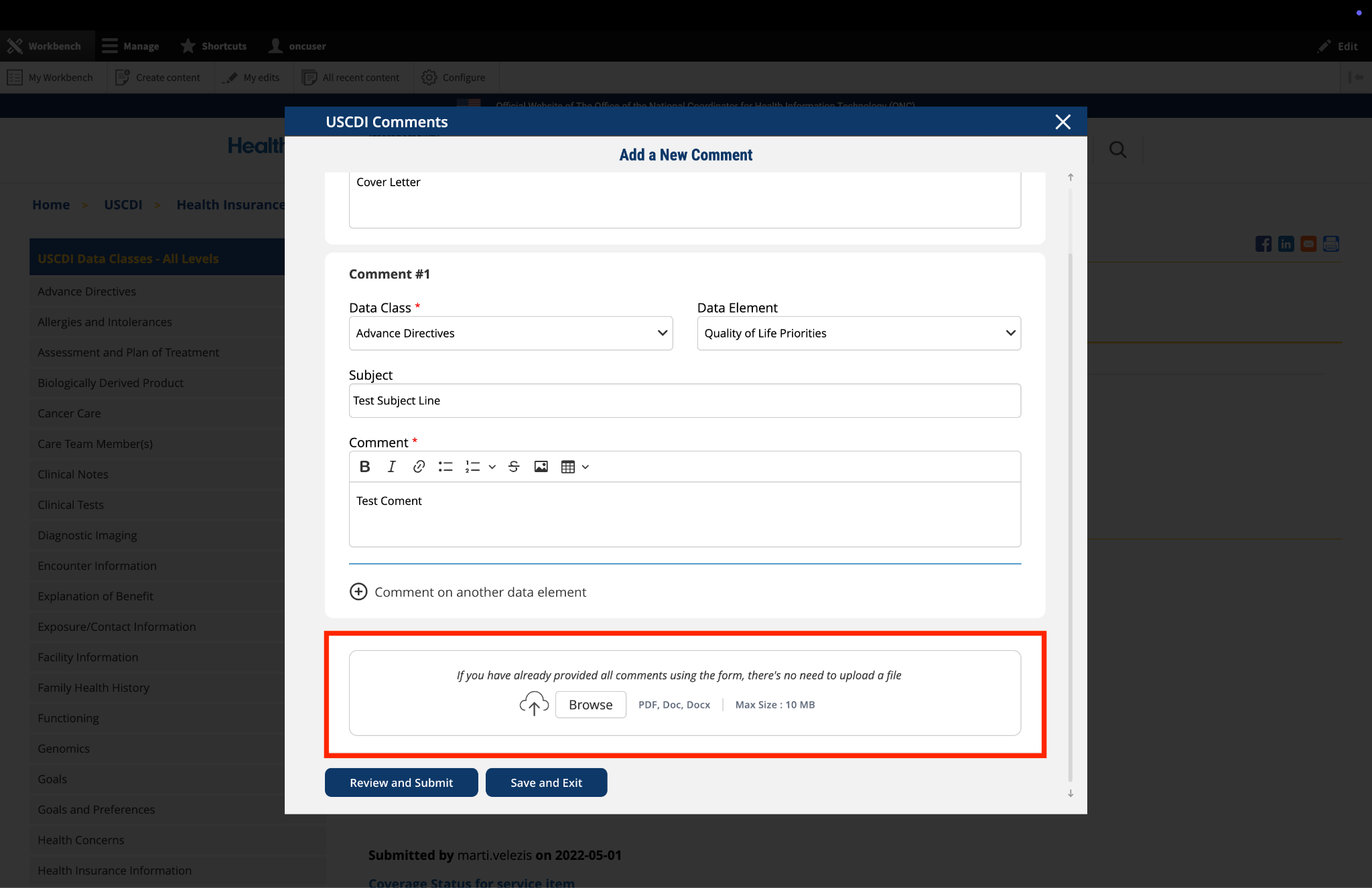
7. Optional: Upload Supporting Files
The platform allows you to upload supporting documentation to enhance your comment:
Locate the "File Upload" section at the bottom of the comment form.
Click to upload any files (such as PDFs or documents) that provide additional context, evidence, or clarification for your comment.
Important: If you have already entered your comments using the form fields, there is no need to upload duplicate content in PDF format. The file upload feature is intended for supplementary materials only. Please avoid uploading files that contain the same information already provided in your comment text.
Fig 4 The "File Upload" section permits users to attach supporting documentation that supplements their written comments.
8. Optional: Save and Exit
If you need to pause your work and return to complete your comment later:
Click the "Save and Exit" button at the bottom of the form.
Your comment will be saved as a draft that you can access and complete later.
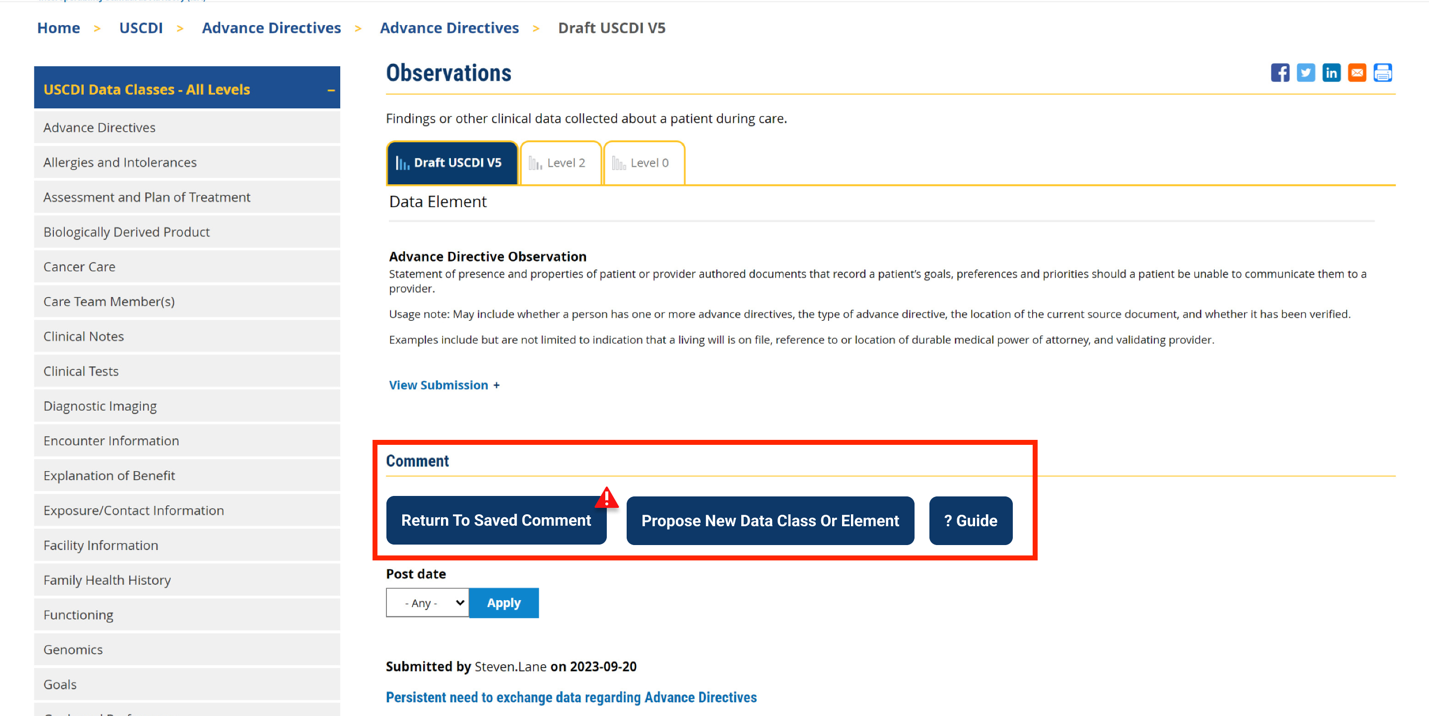
When you return to the platform, you will see a red triangle with an exclamation mark next to the “Return to saved Comment” button, indicating that you have saved comments in draft status.
Click this button to continue working on your draft.
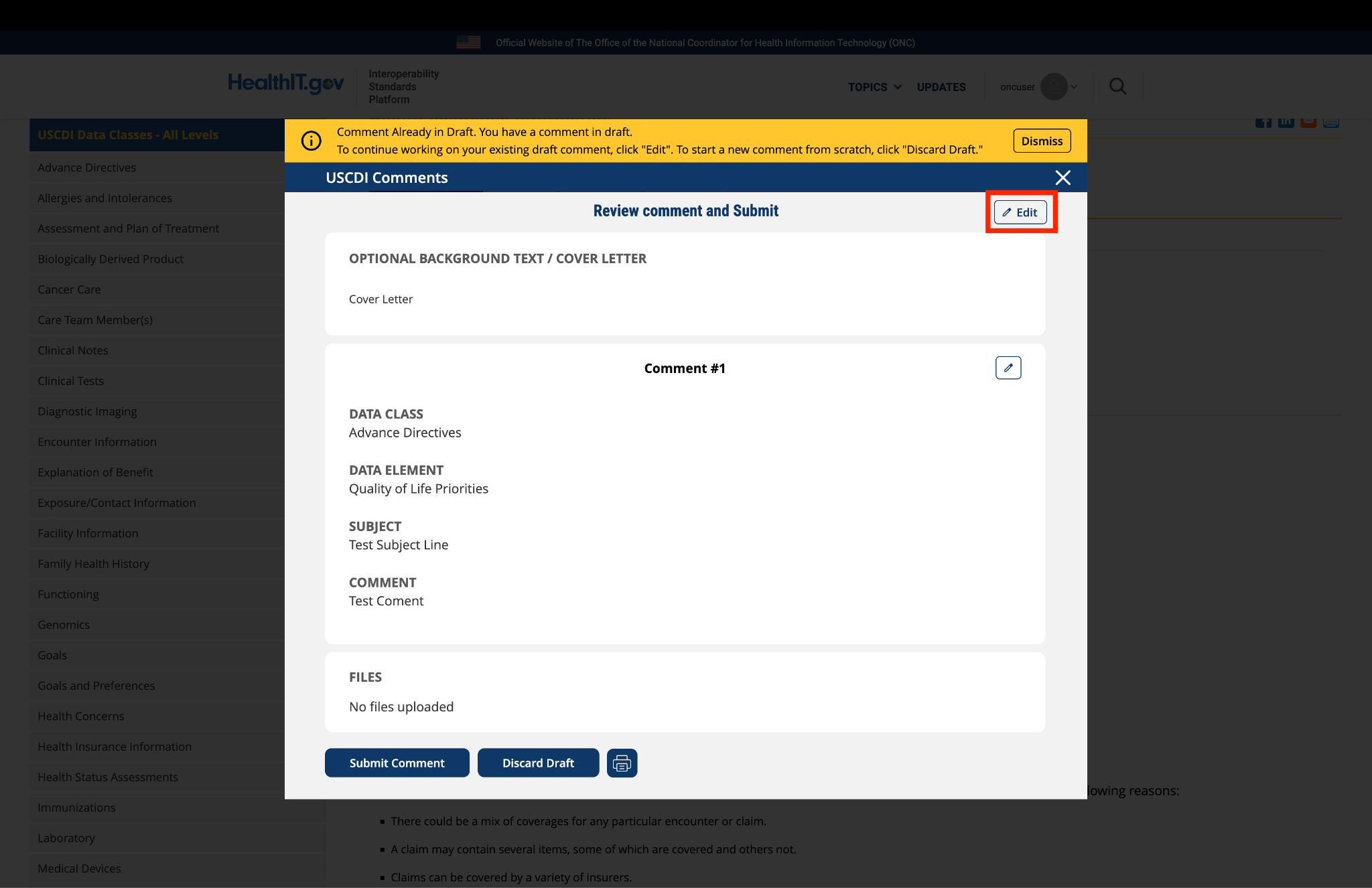
You will be taken to a review page where you can:
Select "Submit Comment" to officially submit your feedback.
Click "Edit" to return to the comment form and make changes
Select "Discard Draft" to delete the saved draft and start fresh
Fig 5 A red triangle with exclamation mark indicator appears next to the “Return to saved Comment” button when draft comments are saved in the system.
9. Review and Submit
Once you have completed your comment:
Click the "Review and Submit" button at the bottom of the form.
This will take you to a review screen displaying your comment(s) in full.
Review all information for accuracy and completeness.
On this review screen, you have three options:
Click "Submit Comment" to officially submit your feedback
Click "Edit" to return to the comment form and make changes
Click "Discard Draft" to delete the comment and start fresh
The review screen also includes a "Print" button that allows you to create a printed copy of your comments for your records.
If you choose to submit, your comment will be recorded in the system and made available for review by the appropriate stakeholders.
Fig 6 The review screen allows users to verify comment content and make any necessary modifications before final submission.


Submitted by RebeccaB on
ASHA: Disability Status and Disability Assessment
ASHA is the national professional, scientific, and credentialing association for 247,000 members, certificate holders, and affiliates who are audiologists; speech-language pathologists (SLPs); speech, language, and hearing scientists; audiology and speech-language pathology assistants; and students. Audiologists specialize in preventing and assessing hearing and balance disorders as well as providing audiologic treatment, including hearing aids. SLPs identify, assess, and treat speech, language, swallowing, and cognitive communication disorders. The American Speech-Language-Hearing Association (ASHA), supports the PACIO Project recommendations to the Office of the National Coordinator for Health Information Technology (ONC) to:
Together, these recommendations address a critical issue in the current structure, which conflates clinician-documented evaluation with patient-reported information and identity, including communication-related disability and access needs, contributing to inconsistency in documentation and its use.
Renaming the existing element to “Disability Assessment” more accurately reflects its function as a clinical evaluation of health status and supports more consistent and appropriate use within care planning and documentation workflows. This is particularly relevant for people with communication-related disabilities, where clinical assessment informs care planning but does not replace patient-reported needs related to communication access. This distinction is necessary for maintaining data integrity and ensuring that assessment data do not serve as proxy for patient-reported demographic information.
Placement of Disability Status within Demographics is necessary to ensure consistent, longitudinal data capture across encounters, providers, and health systems. In contrast to assessment data, which are often episodic and context-dependent, demographic data elements are more reliably exchanged through interoperable systems, including consistent identification of communication access needs across care settings. They are better positioned to support care coordination, population health measurement, and quality reporting.
In addition, aligning Disability Status with the corresponding Accommodations data element within the Demographics data class enhances the operational utility of the data. Structuring both elements at the demographic level enables standardized identification and transmission of accommodation needs across workflows, including intake, triage, and care delivery, and supports implementation through clinical decision support tools, flags, and other health IT functionalities. This is particularly important for people with communication disorders and differences, where timely access to appropriate supports is foundational to safe and effective care.
Collectively, these updates will facilitate more reliable data exchange, reduce variability in documentation practices, and enable more robust analysis of disparities in access, care process, and outcomes for people with disabilities. These changes represent advancements in interoperability, continuity of care, and patient-centered health care delivery.