

United States Core Data for Interoperability (USCDI)
The United States Core Data for Interoperability (USCDI) is a standardized set of health data classes and constituent data elements for nationwide, interoperable health information exchange. Review the USCDI Fact Sheet to learn more.
A USCDI Data Class is an aggregation of Data Elements by a common theme or use case.
A USCDI Data Element is a piece of data defined in USCDI for access, exchange or use of electronic health information.
USCDI ONC New Data Element & Class (ONDEC) Submission System
- USCDI V1
- USCDI V2
- USCDI V3
- USCDI V3.1
- USCDI V4
- USCDI V5
- USCDI V6
- Draft USCDI V7
- Level 2
- Level 1
- Level 0
USCDI V1
Please reference the USCDI version 1 document to the left for applicable standards versions associated with USCDI v1.
Harmful or undesired physiological responses associated with exposure to a substance.
Health professional’s conclusions and working assumptions that will guide treatment of the patient.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Desired state to be achieved by a patient.
Health related matter that is of interest, importance, or worry to someone who may be the patient, patient’s family or patient’s health care provider.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Representing a patient’s smoking behavior.
Unique identifier(s) for a patient's implantable device(s).
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V2
The USCDI v2 contains data classes and elements from USCDI v1 and new data classes and elements submitted through the ONDEC system. Please reference the USCDI Version 2 document to the left for applicable vocabulary standards versions associated with USCDI v2 and to the ONC Standards Bulletin 21-3 for more information about the process to develop USCDI v2 and future versions.
Harmful or undesired physiological responses associated with exposure to a substance.
Health professional’s conclusions and working assumptions that will guide treatment of the patient.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Desired state to be achieved by a patient.
Health related matter that is of interest, importance, or worry to someone who may be the patient, patient’s family or patient’s health care provider.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Representing a patient’s smoking behavior.
Unique identifier(s) for a patient's implantable device(s).
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V3
Please read the USCDI v3 standard document and the ONC Standards Bulletin 22-2 for details. Consistent with EO 14168 and OPM guidance, ASTP/ONC is exercising enforcement and issuing certification guidance for the ONC Health IT Certification Program with respect to certain data elements in USCDI v3. For more information see https://www.healthit.gov/topic/uscdi-v3-data-elements-enforcement-discretion.
Harmful or undesired physiological responses associated with exposure to a substance.
Health professional’s conclusions and working assumptions that will guide treatment of the patient.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Desired state to be achieved by a patient.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Unique identifier(s) for a patient's implantable device(s).
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V3.1
Please read the USCDI v3.1 standard document and the ONC Standards Bulletin 22-2 for details. USCDI version 3.1 updates USCDI version 3 with the following changes: consistent with Executive Order 14168, the Sex, Sexual Orientation, and Gender Identity data elements have been removed or updated in the Patient Demographics/Information Data Class.
Harmful or undesired physiological responses associated with exposure to a substance.
Health professional’s conclusions and working assumptions that will guide treatment of the patient.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Desired state to be achieved by a patient.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Unique identifier(s) for a patient's implantable device(s).
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V4
USCDI v4 added 20 data elements and one data class to USCDI v3. Please reference the USCDI v4 standard document and the ONC Standards Bulletin 23-2 for details. To review the prioritization criteria ONC used to select the USCDI v4 data elements, refer to the ONC Standards Bulletin 22-2.
Harmful or undesired physiological responses associated with exposure to a substance.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Physical place of available services or resources.
Desired state to be achieved by a person or a person’s elections to guide care.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
Information that guides treatment of the patient and recommendations for future treatment.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V5
USCDI v5 was published on July 16, 2024, and includes 16 new data elements and two new data classes. Please read the USCDI v5 standard document and the ONC Standards Bulletin 24-2 for details.
Harmful or undesired physiological responses associated with exposure to a substance.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Physical place of available services or resources.
Desired state to be achieved by a person or a person’s elections to guide care.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Findings or other clinical data collected about a patient during care.
Provider-authored request for the delivery of patient care services.
Usage notes: Orders convey a provider’s intent to have a service performed on or for a patient, or to give instructions on future care.
Data used to categorize individuals for identification, records matching, and other purposes.
Information that guides treatment of the patient and recommendations for future treatment.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V6
ASTP/ONC published USCDI v6 on July 24, 2025, which includes 6 new data elements. Please read the USCDI v6 Standard Document and the ASTP/ONC Standards Bulletin 25-2 for details.
Harmful or undesired physiological responses associated with exposure to a substance.
Information that guides treatment of the patient and recommendations for future treatment.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Physical place of available services or resources.
Family member health condition(s) that are relevant to a patient's care.
Desired state to be achieved by a person or a person’s elections to guide care.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Provider-authored request for the delivery of patient care services.
Usage notes: Orders convey a provider’s intent to have a service performed on or for a patient, or to give instructions on future care.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
Draft USCDI V7
ASTP/ONC published Draft USCDI v7 on January 29, 2026, which includes 30 new data elements. For the official reference, please read the Draft USCDI v7 Standards Document; the ASTP/ONC Standards Bulletin 26-1 provides additional information. ASTP/ONC welcomes input on future versions during the USCDI feedback period, open through April 13, at 11:59 PM ET. During this time, ASTP/ONC is accepting new data element submissions through ONDEC, and comments on data elements may be entered via the updated commenting feature on the USCDI data element pages.
Unintended effects associated with clinical interventions.
Harmful or undesired physiological responses associated with exposure to a substance.
Information that guides treatment of the patient and recommendations for future treatment.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Physical place of available services or resources.
Family member health condition(s) that are relevant to a patient's care.
Desired state to be achieved by a person or a person’s elections to guide care.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Contextual information that provides supporting details for healthcare data.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Provider-authored request for the delivery of patient care services.
Usage notes: Orders convey a provider’s intent to have a service performed on or for a patient, or to give instructions on future care.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
- Represented by a terminology standard or SDO-balloted technical specification or implementation guide.
- Data element is captured, stored, or accessed in multiple production EHRs or other HIT modules from more than one developer.
- Data element is electronically exchanged between more than two production EHRs or other HIT modules of different developers using available interoperability standards.
- Use cases apply to most care settings or specialties.
Level 2
Unintended effects associated with clinical interventions.
Harmful or undesired physiological responses associated with exposure to a substance.
Material substance originating from a biological entity intended to be transplanted or infused into another (possibly the same) biological entity.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Physical place of available services or resources.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Contextual information that provides supporting details for healthcare data.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Provider-authored request for the delivery of patient care services.
Usage notes: Orders convey a provider’s intent to have a service performed on or for a patient, or to give instructions on future care.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
- Represented by a terminology standard or SDO-balloted technical specification or implementation guide.
- Data element is captured, stored, or accessed in at least one production EHR or HIT module.
- Data element is electronically exchanged between two production EHRs or other HIT modules using available interoperability standards.
- Use cases apply to several care settings or specialties.
Level 1
Material substance originating from a biological entity intended to be transplanted or infused into another (possibly the same) biological entity.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Physical place of available services or resources.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Analysis of clinical specimens to obtain information about the health of a patient.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
- Not represented by a terminology standard or SDO-balloted technical specification or implementation guide.
- Data element is captured, stored, or accessed in limited settings such as a pilot or proof of concept demonstration.
- Data element is electronically exchanged in limited environments, such as connectathons or pilots.
- Use cases apply to a limited number of care settings or specialties, or data element represents a specialization of other, more general data elements.
Level 0
Unintended effects associated with clinical interventions.
Harmful or undesired physiological responses associated with exposure to a substance.
Material substance originating from a biological entity intended to be transplanted or infused into another (possibly the same) biological entity.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Health data as reflected in a patient's Explanation of Benefits (EOB) statements, typically derived from claims and other administrative data.
Physical place of available services or resources.
Desired state to be achieved by a patient.
Desired state to be achieved by a person or a person’s elections to guide care.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Findings or other clinical data collected about a patient during care.
Provider-authored request for the delivery of patient care services.
Usage notes: Orders convey a provider’s intent to have a service performed on or for a patient, or to give instructions on future care.
Data used to categorize individuals for identification, records matching, and other purposes.
Information that guides treatment of the patient and recommendations for future treatment.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.

The USCDI ONC New Data Element and Class (ONDEC) Submission System supports a predictable, transparent, and collaborative process, allowing health IT stakeholders to submit new data elements and classes for future versions of USCDI. Click here for more information and to submit new data elements.
The USCDI standard will follow the Standards Version Advancement Process described in the Cures rule to allow health IT developers to update their systems to newer version of USCDI and provide these updates to their customers.
Comment
Submitted by AMIA_Policy on
AMIA USCDI v7 Draft Comments
Please find attached comments on behalf of the American Medical Informatics Association
Submitted by gregthole on
Oracle Health Draft USCDI v7 Comments
Please find attached Oracle Health's comment letter on the draft USCDI v7.
Submitted by LisaRNelsonRI on
Add Generalized Telecom data element
Change Request – Add Generalized Telecom data element to the Healthcare Information Attributes data class
Comment: Make changes to utilize the new Healthcare Information Attributes data class to simplify and standardize all types of telecom data elements into a single data element called Telecom Information within the Healthcare Information Attributes data class.
Rationale: This change would allow the new Healthcare Information Attributes data class to hold generalized data elements that get reused withing other data elements and other data classes, making USCDI more unitary and foundational.
For example, a generic Telecom Information data element could be use to replace the following data elements in the Patient data class: Email Address, Phone Number, Phone Number Type, as well as the Facility Telecom data element in the Facility data class, and the Care Team Member Telecom data element in Care Team Member data class.
Telecom information is needed in so many USCDI data classes. Health Insurance Payers and Health Insurance Plans will need to have Telecom data elements. Encounter Locations may need to include Telecom Information too.
It just seems like a lot of duplication to be proliferating the definition of additional specific Telecom data elements over and over for various particular uses.
Now that the Healthcare Information Attributes data class has been introduced, there’s an opportunity to consolidate repetitious data elements thus removing unnecessary data element bloat and increasing the utility of the USCDI.
Submitted by mturchioe on
ANI comments on USCDI draft v7
The Alliance for Nursing Informatics (ANI) appreciates the opportunity to provide input on the USCDI draft version 7. Please see attached for our complete set of comments.
Submitted by VegaHealth on
Vega Health Comments on USCDI v7
April 13, 2026
The Honorable Thomas Keane, M.D.
National Coordinator for Health IT
U.S. Department of Health and Human Services
220 C St SW
Washington, DC 20201
Re: ONC Standards Bulletin 2026-1 (USCDI Draft Version 7)
Dr. Keane,
Vega Health appreciates the opportunity to provide comments to the Office of the National Coordinator for Health IT’s (ONC’s) bulletin on the United States Core for Data Interoperability Draft Version 7. This draft takes important steps to expand the library of interoperable data elements that underpin clinical technology and innovation. During the review of USCDI v7 and the drafting of future versions, Vega Health urges ONC to consider the following:
- The proposed inclusion of Medication Administration Records as a data element is a key positive development, and ONC should continue to leverage USCDI to make previously unavailable data elements standardized and usable for health system-driven innovation.
Background on Vega Health
Vega Health is dedicated to helping healthcare organizations realize measurable value from healthcare AI. We operate a proprietary platform that connects health systems with a curated marketplace of validated AI solutions created by leading researchers and innovators. We also provide comprehensive integration support and performance monitoring of AI solutions. Our mission is to be the objective, trusted partner equipping health systems everywhere as they scale AI solutions that improve care and operational outcomes.
For health systems, Vega Health provides:
- A proprietary platform that equips healthcare organizations to efficiently run multiple AI solutions within their digital environment;
- A curated marketplace of AI solutions validated in real-world healthcare settings;
- Expert development and implementation support;
- Rigorous measurement and monitoring of clinical outcomes and operational impact; and
- Partnership in co-developing AI solutions optimized for local patient populations.
For healthcare innovators, Vega Health offers:
- Commercialization pathways to scale AI solutions beyond sites of origin;
- Distribution channels to reach health systems seeking validated solutions;
- Implementation expertise to ensure successful deployments in new environments; and
- Transparent monitoring evaluating effectiveness in real-world settings.
Vega Health’s approach to integrating and monitoring AI solutions is built on more than a decade of real-world experience at the Duke Institute for Health Innovation (DIHI) and through the Health AI Partnership (HAIP). At DIHI, our CEO and co-founder Dr. Mark Sendak worked to develop, integrate, and monitor more than 60 AI solutions in live clinical settings at Duke Health. This work included the development of Sepsis Watch, still considered one of the most successful real-world healthcare AI integrations as documented in the peer-reviewed literature.
The work of DIHI and HAIP established foundational frameworks that now guide responsible AI adoption and monitoring across the healthcare industry, including widely cited guidelines for clinical AI integration (the HEAAL framework). HAIP’s work to share best practice frameworks and build an effective practice network beyond academic medical centers – including community hospitals, Federally Qualified Health Centers (FQHCs), and rural health systems – highlighted many of the practical challenges of AI implementation across diverse environments. Vega Health exists to bridge these critical gaps. Many healthcare organizations lack the infrastructure, expertise, and resources to source, integrate, and evaluate the effectiveness of AI solutions. This creates a systemic risk as AI adoption accelerates, threatening to widen a ‘digital divide’ where one class of health systems leverages AI while a second group falls farther behind. We applaud the ONC’s work to reduce the regulatory burden for innovators seeking to assist these healthcare organizations and look forward to this and future opportunities to engage with the agency and its leadership.
Vega Health’s business model operationalizes many of the frameworks promulgated by DIHI and HAIP. Through our platform architecture and monitoring approach, we guide health systems through objective evaluation of technical AI model performance, user adoption and behavior change, and outcome measures. We are committed to acting as an objective third party that provides unbiased performance data to both health systems utilizing AI solutions, as well as the developers of those solutions, all with the goal of advancing innovation.
Vega Health measures performance across four dimensions: technical accuracy/fidelity, user adoption patterns, achievement of clinical/operational outcomes, and return on investment. We implement comprehensive monitoring strategies which use real-world evidence to determine whether an AI solution is delivering value in practice. This approach ensures that performance is evaluated not only in aggregate, but across patient subpopulations. Our team has extensive experience working in clinical settings to evaluate and monitor real-world AI performance, rather than operating at the level of theoretical frameworks.
Vega Health Appreciates Addition of Medication Administration Records Data Element
As ONC continues to advance both the FHIR standard for data exchange and the US Core for Data Interoperability (USCDI) definitions of crucial data elements, Vega Health encourages policymakers to prioritize standardizing elements essential to the implementation of AI/ML solutions in health systems. By rapidly expanding the set of standard data elements at the heart of FHIR-based interoperability, ONC can leverage the health IT certification program to accelerate innovation and avoid the costly and burdensome processes – and potential information blocking abuses – that must be navigated to exchange key data elements unavailable over FHIR.
One pertinent example is Medication Administration Record (MAR) data. From our leadership’s experience implementing AI solutions at multiple health systems, Vega Health has recognized that MAR data are crucial inputs for commonly used clinical AI solutions, such as inpatient deterioration, sepsis prediction, or emergency department likelihood to admit predictive models. MAR specifically captures the actions performed (such as given, on hold, stopped, etc.) with medications prescribed in hospital and ambulatory settings. MAR data is critical for AI solutions that need precise timestamps for when medications are administered and not merely what was ordered. Today, MAR data must be accessed through non-standard means, through custom API infrastructure using obsolete technology dependent on EHR vendors, or via an inconsistent HL7 data feed. Each approach complicates model implementation and requires use of non-standard technology that is poorly documented. Vega Health is encouraged by the inclusion of MAR data in the draft USCDI v7 and encourages ONC to continue expanding the set of standard data elements as a key measure to accelerating the implementation and use of clinical AI solutions.
Conclusion
Vega Health appreciates ONC’s commitment to accelerating the development of USCDI into a standardized dataset that underpins health system-driven informatics and innovation. If Vega Health can be a resource, please do not hesitate to reach out to Vega Health co-founder and CEO Mark Sendak (Mark.Sendak@vegahealth.com).
Sincerely,
Mark Sendak, MD, MPP
Co-founder and CEO, Vega Health
Submitted by Allina Health … on
Allina Health Comments on USCDI Draft v7
Allina Health appreciates the opportunity to provide the attached comments to ONC in response to the draft USCDI Version 7.
Submitted by Hiral on
UI Health Public Feedback: Draft USCDI Version 7
UI Health appreciates this opportunity to provide feedback on the draft USCDI version 7. Please see attached for details.
Submitted by Jennifer Holloman on
American Hospital Association (AHA) Comments for USCDI v7
Please see link below to American Hospital Association (AHA) comments for USCDI v7:
Submitted by Elza Black on
FAH Comments on USCDI V7
The Federation of American Hospitals (FAH) appreciates the opportunity to provide feedback on the Draft USCDI Version 7. Our comments may be found at the following link: FAH-USCDI-Comment-Letter-4.13.26.pdf
Help
1. Optional: Background Text / Cover Letter
The "Optional Background Text / Cover Letter" field provides space for additional context or introductory information related to your comment.
If you wish to provide context, explanation, or an introduction to your comment, enter this information in the field labeled "Optional Background Text / Cover Letter." This is entirely optional and is most useful when submitting multiple related comments or when additional background would help reviewers understand your feedback.
If you are only commenting on a single data class or element, you may leave this field blank.
2. Select the Data Class
To specify which data class your comment addresses:
- In the "Data Class" drop-down menu, select the appropriate data class you want to comment on.
- If you are providing a general comment that is not specific to a data element, select "General" from the options. Comments with this designation will be displayed on the USCDI landing page.
- Note that the Data Class field will automatically populate based on your current location in the platform:
- If you are on a data class page, the field will be set to that specific data class
- If you are on a data element page, the corresponding data class will be pre-selected
3. Select the Data Element
To specify which data element your comment addresses:
- In the "Data Element" drop-down menu, select the specific data element you want to comment on.
- The drop-down menu will display only the elements available under the data class you selected in the previous step.
- You can use the search function within the drop-down to quickly locate a specific data element.
- If you are commenting on the data class itself rather than a specific element, you may leave this field blank.
Note: Comments on a specific data element will appear on the respective data element page, while comments on a data class (without a specific element selected) will appear on the landing page for that data class.
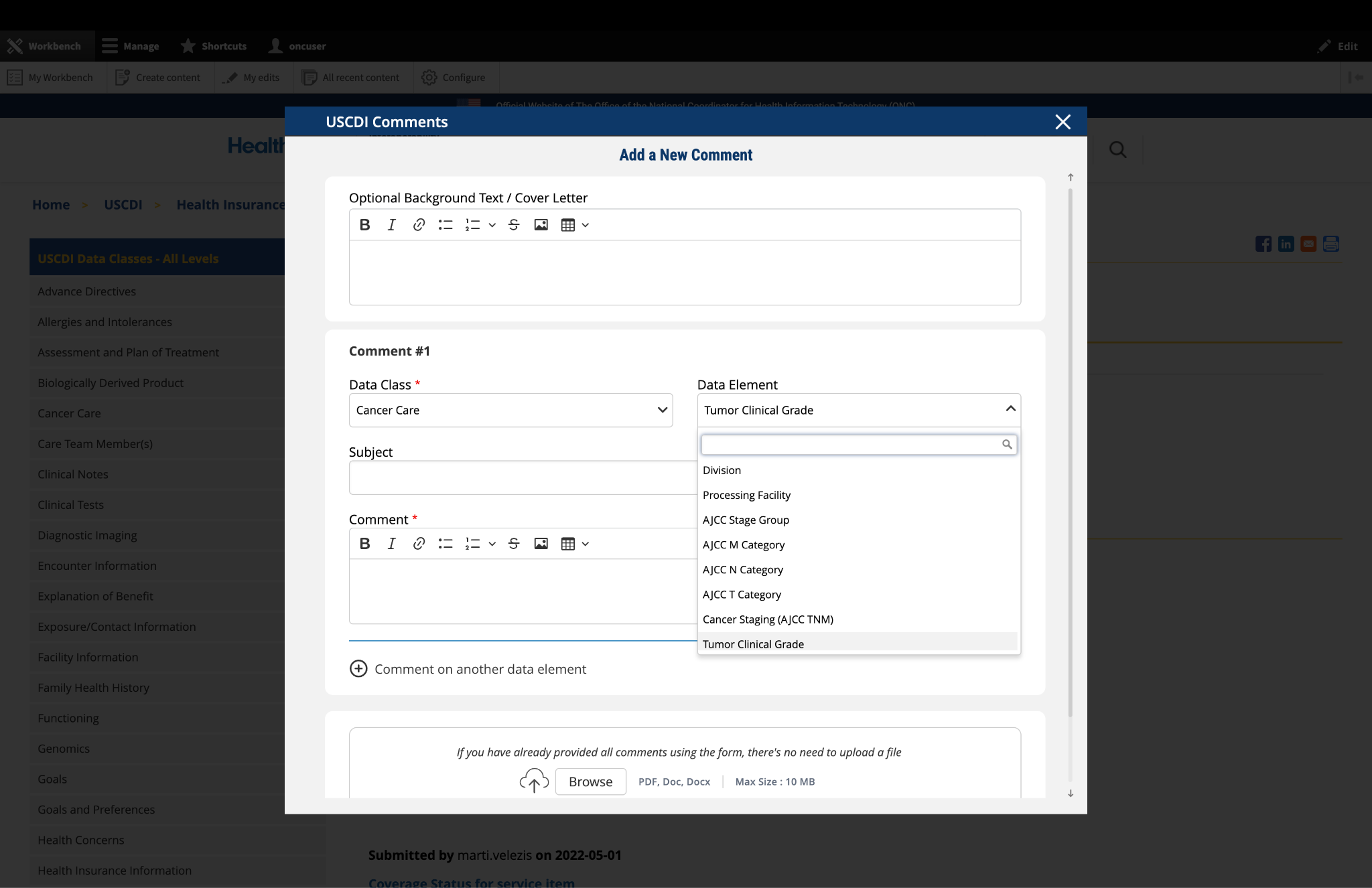
Fig 1 The "Data Class" and "Data Element" dropdown menus allow users to specify the exact content they wish to comment on.
4. Optional: Propose New Data Class or Element
If you cannot find the appropriate data class or element for your comment:
- Instead of clicking the "Comment On An Existing Data Class Or Element" button, click the adjacent button labeled "Propose a New Data Class or Data Element."
- This will redirect you to the ONDEC (ONC New Data Element and Class) Submission System.
- In the ONDEC system, follow the provided instructions to submit your proposal for a new data class or element.
- Once your proposal is submitted through ONDEC, it will be reviewed separately from the commenting process.
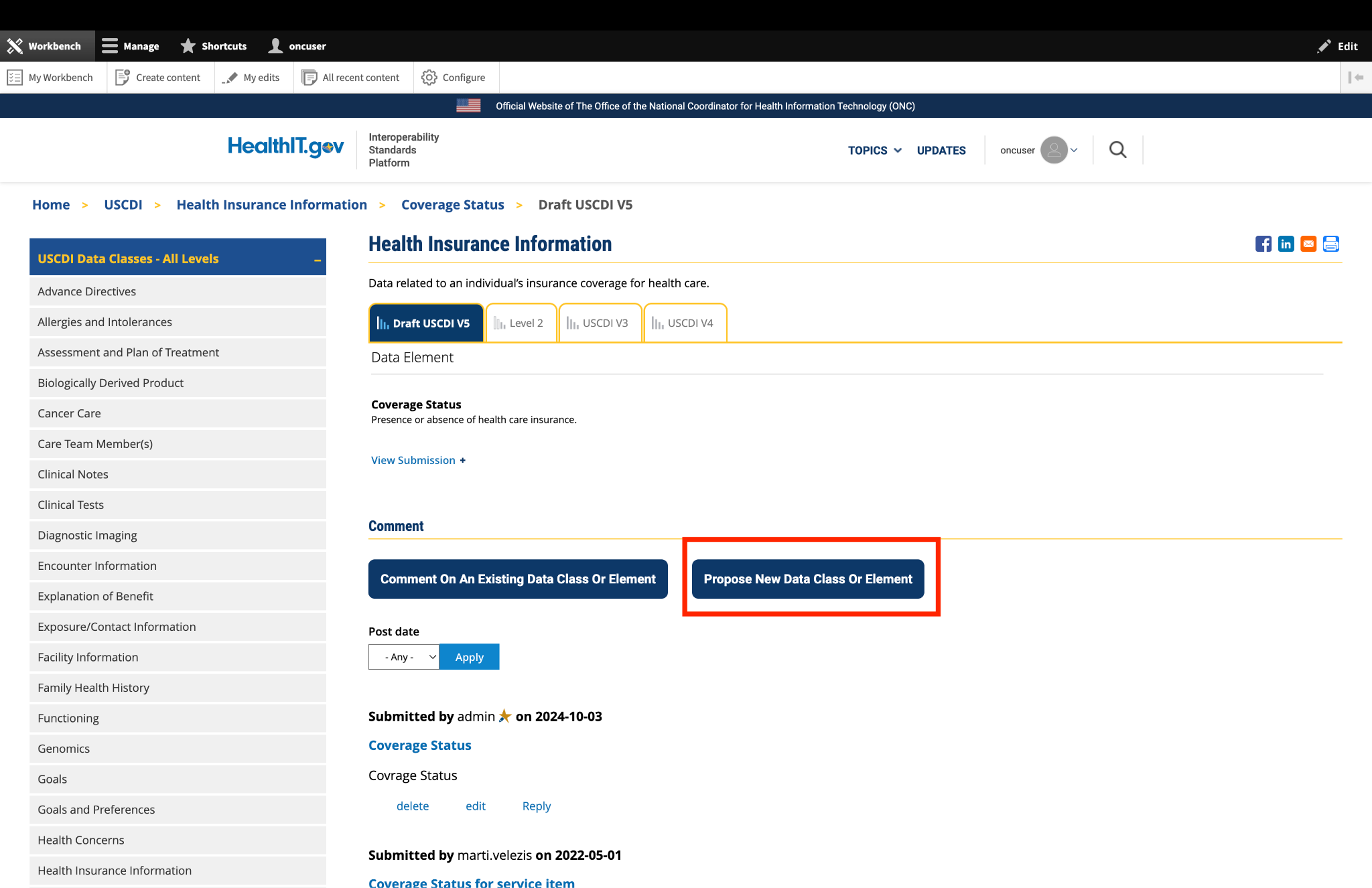
Fig 2 The "Propose a New Data Class or Data Element" button redirects users to the ONDEC Submission System for proposing new data elements not currently available in the system.
5. Complete the Comment Form
Fill out the required fields in the comment form:
Subject: Enter a brief, descriptive title that summarizes your comment. This helps reviewers quickly understand the nature of your feedback.
Comment: In this field, provide the full details of your comment or feedback. Be as clear and specific as possible about your suggestions, concerns, or observations. Include any relevant details that support your position.
6. Optional: Add Additional Comments
If you need to comment on multiple data classes or elements:
- After completing your first comment, click the link labeled "Comment on another data element" at the bottom of the form.
- A new comment section will appear, allowing you to enter details for your additional comment.
- For each additional comment, you must select the appropriate data class and data element from the drop-down menus.
- Complete the Subject and Comment fields for your additional comment.
- Repeat this process for each additional comment you wish to submit.
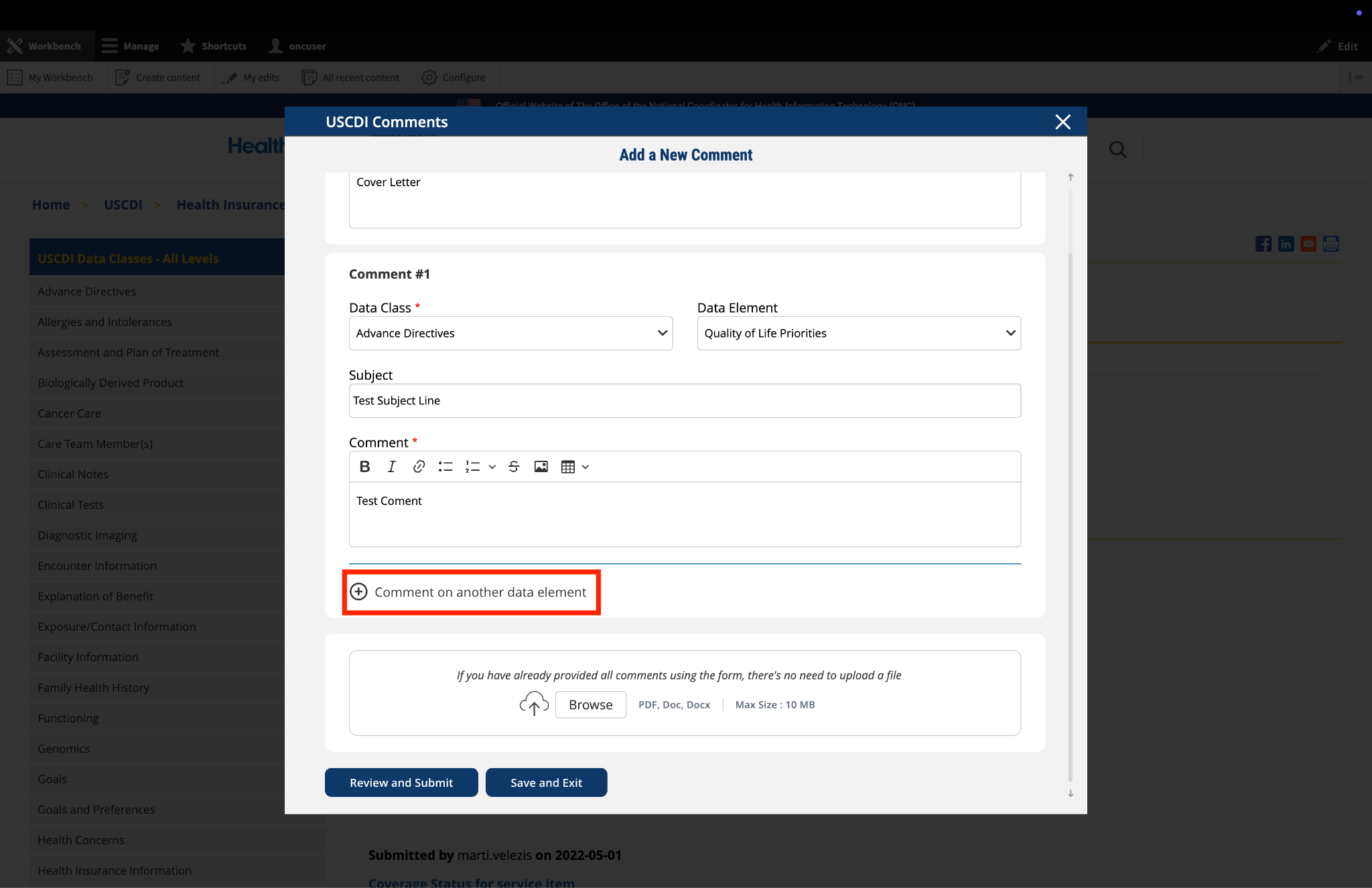
Fig 3 The "Comment on another data element" link enables users to create multiple comments addressing different elements within a single submission.
7. Optional: Upload Supporting Files
The platform allows you to upload supporting documentation to enhance your comment:
- Locate the "File Upload" section at the bottom of the comment form.
- Click to upload any files (such as PDFs or documents) that provide additional context, evidence, or clarification for your comment.
Important: If you have already entered your comments using the form fields, there is no need to upload duplicate content in PDF format. The file upload feature is intended for supplementary materials only. Please avoid uploading files that contain the same information already provided in your comment text.
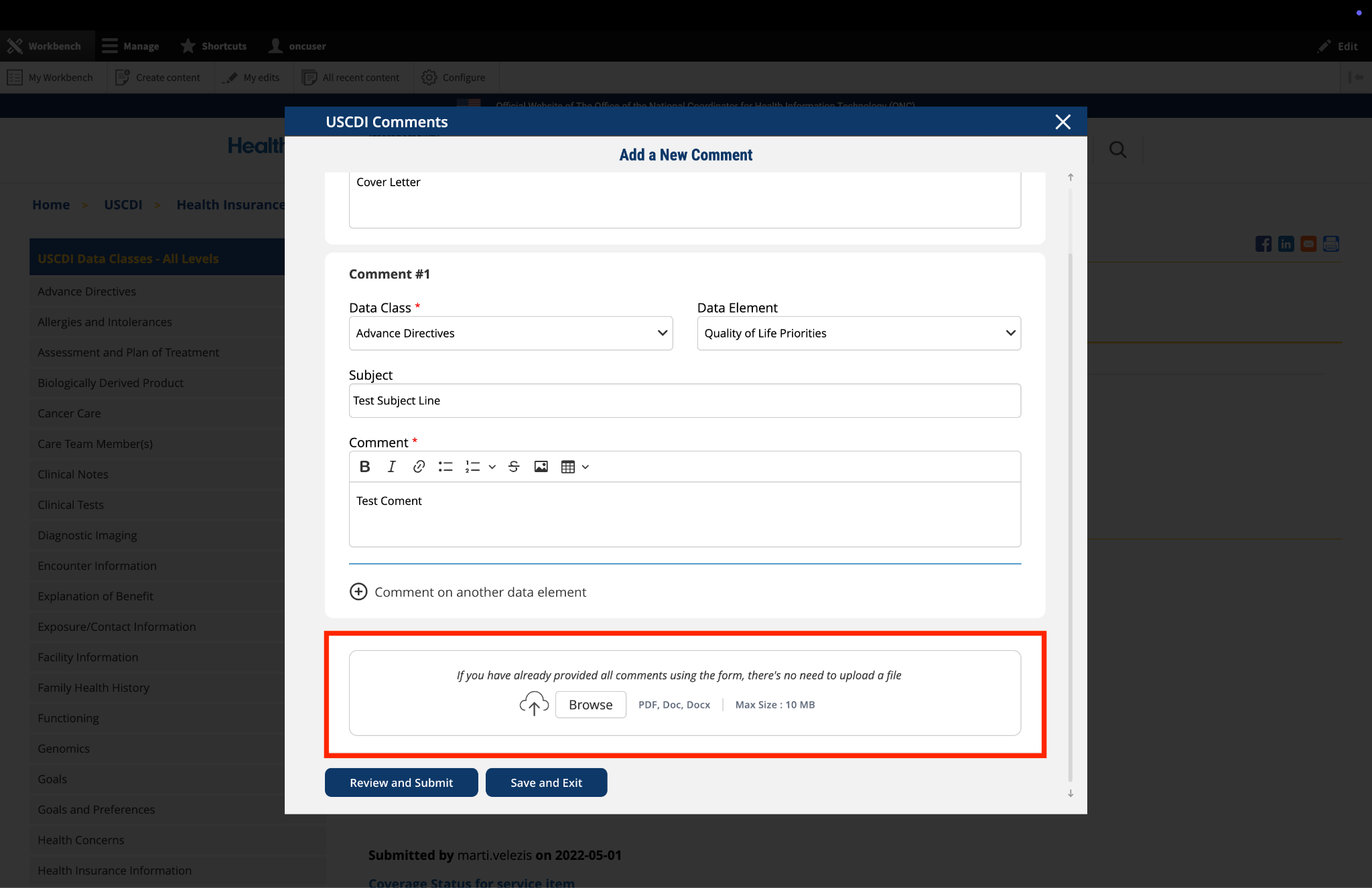
Fig 4 The "File Upload" section permits users to attach supporting documentation that supplements their written comments.
8. Optional: Save and Exit
If you need to pause your work and return to complete your comment later:
- Click the "Save and Exit" button at the bottom of the form.
- Your comment will be saved as a draft that you can access and complete later.
- When you return to the platform, you will see a red triangle with an exclamation mark next to the “Return to saved Comment” button, indicating that you have saved comments in draft status.
- Click this button to continue working on your draft.
- You will be taken to a review page where you can:
- Select "Submit Comment" to officially submit your feedback.
- Click "Edit" to return to the comment form and make changes
- Select "Discard Draft" to delete the saved draft and start fresh
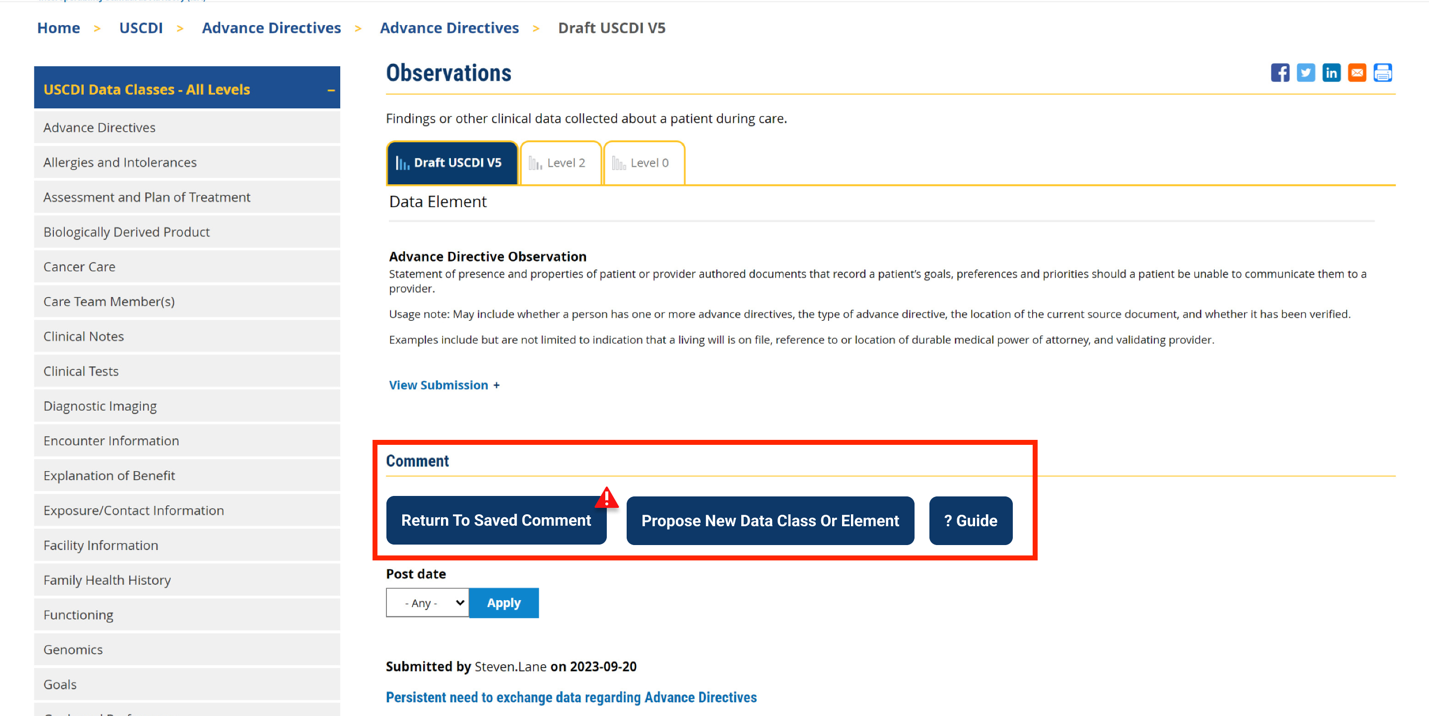
Fig 5 A red triangle with exclamation mark indicator appears next to the “Return to saved Comment” button when draft comments are saved in the system.
9. Review and Submit
Once you have completed your comment:
- Click the "Review and Submit" button at the bottom of the form.
- This will take you to a review screen displaying your comment(s) in full.
- Review all information for accuracy and completeness.
- On this review screen, you have three options:
- Click "Submit Comment" to officially submit your feedback
- Click "Edit" to return to the comment form and make changes
- Click "Discard Draft" to delete the comment and start fresh
- The review screen also includes a "Print" button that allows you to create a printed copy of your comments for your records.
- If you choose to submit, your comment will be recorded in the system and made available for review by the appropriate stakeholders.
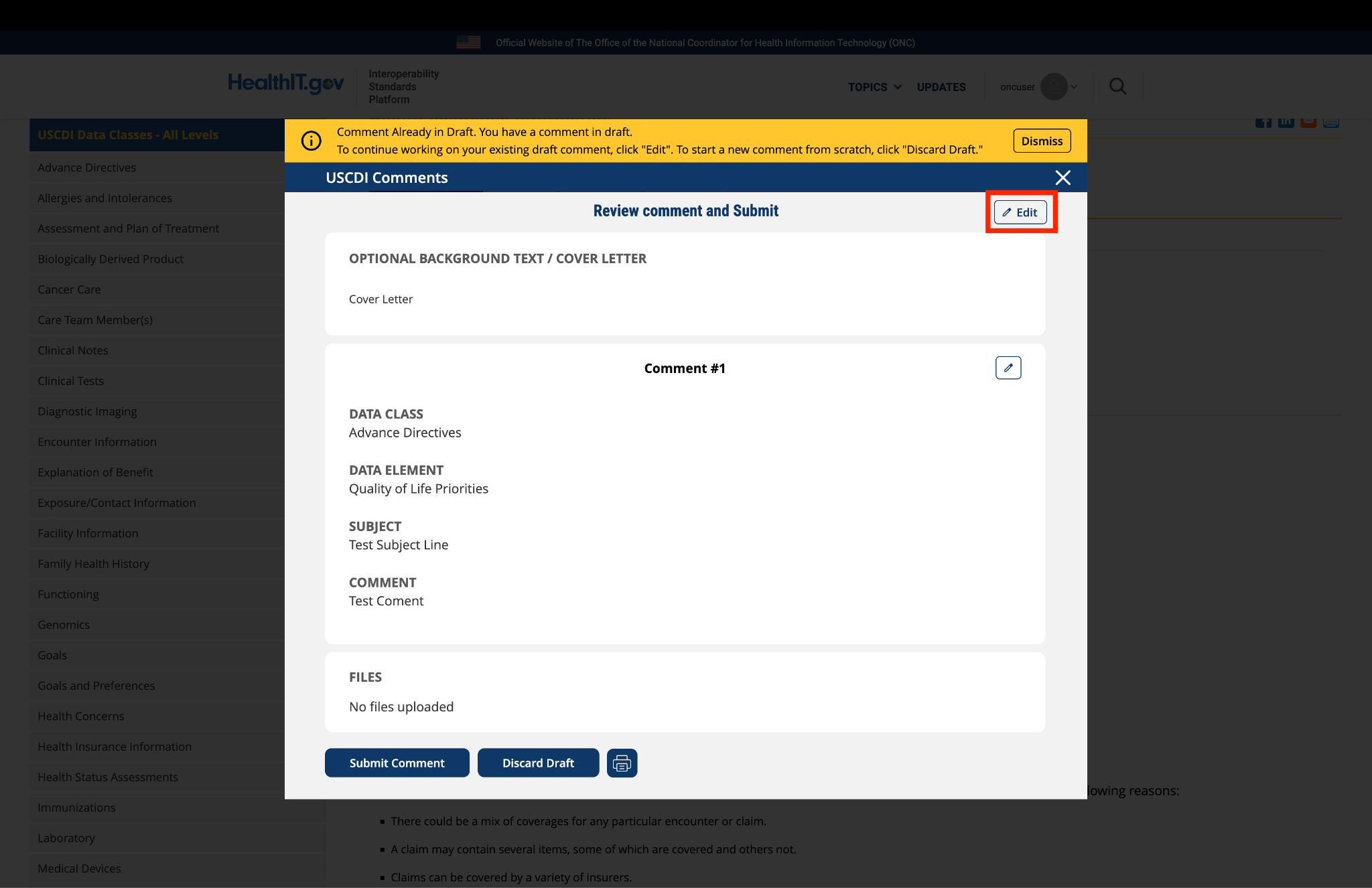
Fig 6 The review screen allows users to verify comment content and make any necessary modifications before final submission.
Submitted by markaroberts85 on
CARIN Alliance Comments on USCDI V7
The CARIN Alliance thanks you for the opportunity to provide feedback on USCDI draft version 7. As you are aware, the CARIN Alliance is a multi-sector group of stakeholders representing numerous hospitals, thousands of physicians, and millions of consumers and caregivers. We are committed to ensuring that consumers and their authorized caregivers can securely access their health information, including electronic health information, through modern technology protocols, the use of digital identity, and the advancement of open, industry‑adopted standards.
The CARIN Alliance has consistently advocated for the inclusion of the data elements from the Common Payer Consumer Data Set (CPCDS), which is core to the FHIR®-based CARIN IG for Blue Button®, to be included in USCDI versions 2, 3, 4, 5, and 6. These elements, which are not all included in USCDI, are essential to advancing the Office of the National Coordinator for Health IT’s (ONC) mission of establishing “a standardized set of health data classes and constituent data elements for nationwide, interoperable health information exchange.”
Please find our comments attached.