

United States Core Data for Interoperability (USCDI)
The United States Core Data for Interoperability (USCDI) is a standardized set of health data classes and constituent data elements for nationwide, interoperable health information exchange. Review the USCDI Fact Sheet to learn more.
A USCDI Data Class is an aggregation of Data Elements by a common theme or use case.
A USCDI Data Element is a piece of data defined in USCDI for access, exchange or use of electronic health information.
USCDI ONC New Data Element & Class (ONDEC) Submission System
- USCDI V1
- USCDI V2
- USCDI V3
- USCDI V3.1
- USCDI V4
- USCDI V5
- USCDI V6
- Draft USCDI V7
- Level 2
- Level 1
- Level 0
USCDI V1
Please reference the USCDI version 1 document to the left for applicable standards versions associated with USCDI v1.
Harmful or undesired physiological responses associated with exposure to a substance.
Health professional’s conclusions and working assumptions that will guide treatment of the patient.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Desired state to be achieved by a patient.
Health related matter that is of interest, importance, or worry to someone who may be the patient, patient’s family or patient’s health care provider.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Representing a patient’s smoking behavior.
Unique identifier(s) for a patient's implantable device(s).
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V2
The USCDI v2 contains data classes and elements from USCDI v1 and new data classes and elements submitted through the ONDEC system. Please reference the USCDI Version 2 document to the left for applicable vocabulary standards versions associated with USCDI v2 and to the ONC Standards Bulletin 21-3 for more information about the process to develop USCDI v2 and future versions.
Harmful or undesired physiological responses associated with exposure to a substance.
Health professional’s conclusions and working assumptions that will guide treatment of the patient.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Desired state to be achieved by a patient.
Health related matter that is of interest, importance, or worry to someone who may be the patient, patient’s family or patient’s health care provider.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Representing a patient’s smoking behavior.
Unique identifier(s) for a patient's implantable device(s).
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V3
Please read the USCDI v3 standard document and the ONC Standards Bulletin 22-2 for details. Consistent with EO 14168 and OPM guidance, ASTP/ONC is exercising enforcement and issuing certification guidance for the ONC Health IT Certification Program with respect to certain data elements in USCDI v3. For more information see https://www.healthit.gov/topic/uscdi-v3-data-elements-enforcement-discretion.
Harmful or undesired physiological responses associated with exposure to a substance.
Health professional’s conclusions and working assumptions that will guide treatment of the patient.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Desired state to be achieved by a patient.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Unique identifier(s) for a patient's implantable device(s).
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V3.1
Please read the USCDI v3.1 standard document and the ONC Standards Bulletin 22-2 for details. USCDI version 3.1 updates USCDI version 3 with the following changes: consistent with Executive Order 14168, the Sex, Sexual Orientation, and Gender Identity data elements have been removed or updated in the Patient Demographics/Information Data Class.
Harmful or undesired physiological responses associated with exposure to a substance.
Health professional’s conclusions and working assumptions that will guide treatment of the patient.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Desired state to be achieved by a patient.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Unique identifier(s) for a patient's implantable device(s).
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V4
USCDI v4 added 20 data elements and one data class to USCDI v3. Please reference the USCDI v4 standard document and the ONC Standards Bulletin 23-2 for details. To review the prioritization criteria ONC used to select the USCDI v4 data elements, refer to the ONC Standards Bulletin 22-2.
Harmful or undesired physiological responses associated with exposure to a substance.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Physical place of available services or resources.
Desired state to be achieved by a person or a person’s elections to guide care.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
Information that guides treatment of the patient and recommendations for future treatment.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V5
USCDI v5 was published on July 16, 2024, and includes 16 new data elements and two new data classes. Please read the USCDI v5 standard document and the ONC Standards Bulletin 24-2 for details.
Harmful or undesired physiological responses associated with exposure to a substance.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Physical place of available services or resources.
Desired state to be achieved by a person or a person’s elections to guide care.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Findings or other clinical data collected about a patient during care.
Provider-authored request for the delivery of patient care services.
Usage notes: Orders convey a provider’s intent to have a service performed on or for a patient, or to give instructions on future care.
Data used to categorize individuals for identification, records matching, and other purposes.
Information that guides treatment of the patient and recommendations for future treatment.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V6
ASTP/ONC published USCDI v6 on July 24, 2025, which includes 6 new data elements. Please read the USCDI v6 Standard Document and the ASTP/ONC Standards Bulletin 25-2 for details.
Harmful or undesired physiological responses associated with exposure to a substance.
Information that guides treatment of the patient and recommendations for future treatment.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Physical place of available services or resources.
Family member health condition(s) that are relevant to a patient's care.
Desired state to be achieved by a person or a person’s elections to guide care.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Provider-authored request for the delivery of patient care services.
Usage notes: Orders convey a provider’s intent to have a service performed on or for a patient, or to give instructions on future care.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
Draft USCDI V7
ASTP/ONC published Draft USCDI v7 on January 29, 2026, which includes 30 new data elements. For the official reference, please read the Draft USCDI v7 Standards Document; the ASTP/ONC Standards Bulletin 26-1 provides additional information. ASTP/ONC welcomes input on future versions during the USCDI feedback period, open through April 13, at 11:59 PM ET. During this time, ASTP/ONC is accepting new data element submissions through ONDEC, and comments on data elements may be entered via the updated commenting feature on the USCDI data element pages.
Unintended effects associated with clinical interventions.
Harmful or undesired physiological responses associated with exposure to a substance.
Information that guides treatment of the patient and recommendations for future treatment.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Physical place of available services or resources.
Family member health condition(s) that are relevant to a patient's care.
Desired state to be achieved by a person or a person’s elections to guide care.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Contextual information that provides supporting details for healthcare data.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Provider-authored request for the delivery of patient care services.
Usage notes: Orders convey a provider’s intent to have a service performed on or for a patient, or to give instructions on future care.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
- Represented by a terminology standard or SDO-balloted technical specification or implementation guide.
- Data element is captured, stored, or accessed in multiple production EHRs or other HIT modules from more than one developer.
- Data element is electronically exchanged between more than two production EHRs or other HIT modules of different developers using available interoperability standards.
- Use cases apply to most care settings or specialties.
Level 2
Unintended effects associated with clinical interventions.
Harmful or undesired physiological responses associated with exposure to a substance.
Material substance originating from a biological entity intended to be transplanted or infused into another (possibly the same) biological entity.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Physical place of available services or resources.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Contextual information that provides supporting details for healthcare data.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Provider-authored request for the delivery of patient care services.
Usage notes: Orders convey a provider’s intent to have a service performed on or for a patient, or to give instructions on future care.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
- Represented by a terminology standard or SDO-balloted technical specification or implementation guide.
- Data element is captured, stored, or accessed in at least one production EHR or HIT module.
- Data element is electronically exchanged between two production EHRs or other HIT modules using available interoperability standards.
- Use cases apply to several care settings or specialties.
Level 1
Material substance originating from a biological entity intended to be transplanted or infused into another (possibly the same) biological entity.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Physical place of available services or resources.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Analysis of clinical specimens to obtain information about the health of a patient.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
- Not represented by a terminology standard or SDO-balloted technical specification or implementation guide.
- Data element is captured, stored, or accessed in limited settings such as a pilot or proof of concept demonstration.
- Data element is electronically exchanged in limited environments, such as connectathons or pilots.
- Use cases apply to a limited number of care settings or specialties, or data element represents a specialization of other, more general data elements.
Level 0
Unintended effects associated with clinical interventions.
Harmful or undesired physiological responses associated with exposure to a substance.
Material substance originating from a biological entity intended to be transplanted or infused into another (possibly the same) biological entity.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Health data as reflected in a patient's Explanation of Benefits (EOB) statements, typically derived from claims and other administrative data.
Physical place of available services or resources.
Desired state to be achieved by a patient.
Desired state to be achieved by a person or a person’s elections to guide care.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Findings or other clinical data collected about a patient during care.
Provider-authored request for the delivery of patient care services.
Usage notes: Orders convey a provider’s intent to have a service performed on or for a patient, or to give instructions on future care.
Data used to categorize individuals for identification, records matching, and other purposes.
Information that guides treatment of the patient and recommendations for future treatment.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.

The USCDI ONC New Data Element and Class (ONDEC) Submission System supports a predictable, transparent, and collaborative process, allowing health IT stakeholders to submit new data elements and classes for future versions of USCDI. Click here for more information and to submit new data elements.
The USCDI standard will follow the Standards Version Advancement Process described in the Cures rule to allow health IT developers to update their systems to newer version of USCDI and provide these updates to their customers.
Comment
Submitted by rdillaire on
CMS-CCSQ supports "Veteran Confirmation Flag" ONDEC submission
CMS-CCSQ supports the ONDEC submission for the new "Veteran Confirmation Flag" data element proposed by the VA.
Recommendation: CMS CCSQ recommends the Veteran Confirmation Flag data element be included in the Patient Demographics/Information data class in Level 2 of USCDI.
Rationale: CMS CCSQ is requesting that Veteran Confirmation Flag be added to Level 2 of USCDI under the Patient Demographics/Information data class. Veteran Confirmation Flag is a critical data element that identifies a high-priority population that served in active military, naval, air, or space service, and who was discharged or released under conditions other than dishonorable, as defined in USC Title 38 Veteran. This data is essential for recognizing the unique healthcare needs of Veterans and their eligibility for specialized programs, such as behavioral health screenings and military toxic exposure evaluations under initiatives like the Promise to Address Comprehensive Toxics (PACT) Act. The inclusion of this data in USCDI would ensure that Veterans receive the necessary care and services, particularly when receiving care outside of Veterans Administration (VA) facilities. This is increasingly important as veterans are more frequently seeking care outside of VA facilities, so identifying Veteran Confirmation Flag is critical for facilitating coordination of care and follow-up. The Veteran Confirmation Flag is available through a VA-provided API that can be queried on demand during intake, in urgent care or emergency department workflows, or through batch queries for scheduled visits.
Including Veteran Confirmation Flag in USCDI aligns with the broader goals of improving care for underserved populations, as it enables clinicians to tailor interventions to the specific needs of Veterans. By incorporating this data into the Patient Demographics category, providers will be able to leverage it for clinical decision support, such as triggering specialized interventions or referrals. Additionally, it supports administrative workflows like benefit eligibility reporting and quality measure assessments.
The ability to track and stratify Veteran Confirmation Flag ensures that Veterans receive appropriate care regardless of their care setting, whether transitioning from a VA facility to a community hospital or receiving care from multiple providers. This inclusion helps reduce the risks veterans may face from receiving fragmented care across various providers and will also enhance interoperability, ensuring that Veteran Confirmation Status is accurately exchanged across disparate healthcare systems, promoting coordinated care and continuity.
Technically, Veteran Confirmation Flag has already been implemented in production environments, such as Epic and Oracle Cerner, proving its broad applicability. By formalizing Veteran Confirmation Flag in USCDI, we not only ensure Veterans receive the care they are entitled to but also support the ongoing efforts to reduce healthcare disparities and improve overall care quality for this high-priority population.
Submitted by Solarf3050 on
HL7 Comments on Draft USCDI v7
Please see attached the comments of Health Level Seven (HL7) International on the Draft United States Core Data for Interoperability Version 7 (Draft USCDI v7). We appreciate the opportunity to provide feedback!
Submitted by shannon.vogel@… on
TMA Comments on Draft USCDI Version 7
The Texas Medical Association appreciates the opportunity to provide the attached comments to ONC on draft USCDI Version 7.
Submitted by knicholoff@ehra.org on
EHR Association Comments on Draft USCDI v7
The HIMSS Electronic Health Record (EHR) Association appreciates the opportunity to provide feedback on the draft USCDI Version 7. Our comments are attached.
Submitted by Riki Merrick on
SHIELD USCDI V7 Draft Overarching comments
- SHIELD appreciates the role that USCDI plays in standardizing health data for interoperability. However, the use of classes for grouping of the data elements results in a fragmentation of data elements that are applicable to particular use cases, and might “hide” important elements in classes not familiar to the implementers of the use case. At least for the clinical elements SHIELD suggests to remove the classes and provide a listing of the elements alphabetically. Then, for example in USCDI+, each use case or speciality could identify the USCDI elements that are required to preserve the clinical context. Specifically for the laboratory data use case the fragmentation of required elements for orders and results across 7 of these classes leads to different interpretations of the requirements. SHIELD participants have noted that without a complete set of laboratory data, they are unable to validate and therefore integrate the laboratory data that is currently flowing into care processes and analytics, resulting in low-yield, low quality data exchanges.
- The high level of USCDI element definitions leads to inconsistencies across the industry when individual health and laboratory entities determine individually how to fill in the gaps. The lack of a coherent data model is still a barrier to end to end laboratory interoperability and SHIELD strongly encourages ASTP/ONC to consider more formally defining a data model for the current lab related data elements, including more formal vocabulary bindings. By providing a more defined data model, boundaries and relationships between similar elements such as Device Type vs UDI, Encounter vs Appointment; Procedures vs Orders; and Events vs Outcomes would become clearer. This would add great value by improving laboratory data interoperability and could be an opportunity to onboard Laboratory Information Systems into FHIR data exchange with standardized source data. SHIELD would be excited to offer its industry, informatics and healthcare expertise to any effort to build out a shared laboratory data model with other laboratory interoperability stakeholders.
- SHIELD suggests the support for synonyms for USCDI data elements, to enable specialities to utilize the names familiar in their domain to enable proper identification of a data element; for example while the usage notes include the synoym of Specimen Collection Date/Time, a laboratorian may not even look at the element because of the non-intuitive name Performance Time.
- SHIELD suggests to update to the latest available version at time of publication of V7 for all called out coding systems/terminologies.
Submitted by Sasha_TerMaat on
Submitted by krystal.burke@… on
Please see our file upload…
Please see our file upload for full comment.
Submitted by molenda on
Anatomic Localization
Thank you for the opportunity to comment on Draft Version 7 of the United States Core Data for Interoperability (USCDI).
Anatomy Mapper OpCo is an anatomical intelligence company focused on maintaining standardized, interoperable, and clinically usable representations of anatomy for healthcare workflows. Our platform supports visual, descriptive, standardized, and codeable site selection in clinical workflows, helping improve anatomical precision, data quality, understandability, and interoperability.
We appreciate ASTP/ONC's continued work to advance USCDI as a national foundation for interoperable health information exchange. By establishing a standardized set of core data elements, USCDI promotes greater consistency, clearer semantics, and more clinically meaningful exchange across healthcare stakeholders. Draft USCDI v7 continues that progress through thoughtful additions across orders, procedures, diagnostic imaging, healthcare information attributes, and other data classes.
We respectfully recommend that ASTP/ONC consider Anatomic Localization as a cross-cutting concept relevant to many existing and proposed USCDI data classes. In many clinical workflows, it is not enough to know that a procedure, order, finding, or event occurred. It is also necessary to know where on the patient's body it occurred in a standardized, unambiguous, and machine-readable way. (Note: "Anatomic Localization" was suggested over "Anatomic Location" because there is already a proposed data element "Location of Procedure" that deals with Place of Service. However, "Anatomic Location" could be substituted.)
This concept is relevant across numerous data classes, including but not limited to:
- Procedures
- Orders
- Adverse Events
- Clinical Notes
- Healthcare Information Attributes
- Problems
- Clinical Tests
- Diagnostic Imaging
- Laboratory, including Specimen Source Site
For example, anatomical localization is often essential to distinguish between otherwise similar procedures, orders, findings, and reports. It supports safer and more precise routing, scheduling, documentation, result interpretation, referral workflows, and longitudinal tracking. In particular, a canonical, interoperable anatomical vocabulary would improve clarity where existing Applicable Vocabulary Standards are broad, where multiple concepts overlap in meaning for the same anatomical localization, or where anatomical detail is variably represented.
We therefore encourage ASTP/ONC to consider one of two approaches:
1. Add Anatomic Localization as a reusable data element that can be applied across multiple data classes and data elements; or
2. Create a dedicated data class for anatomy, such as Surface Anatomy, with Anatomic Localization as a principal data element that can also be reused across other classes.
A concise definition could be:
Anatomic Localization: A standardized, codeable representation of a patient body site used to localize clinical findings, procedures, specimens, orders, and other health information; includes a canonical site identifier and laterality when applicable.
At minimum, such an element could support:
- a standardized site identifier,
- laterality when relevant,
- human-readable display text,
- optional attributes (composable codes, coordinates, images, etc), and
- the ability to represent coarse or fine-grained anatomical specificity depending on feasibility and workflow needs.
We believe this would strengthen USCDI’s support for clinically meaningful interoperability and help fill an important semantic gap across multiple existing classes and data elements. In particular, it may improve the usability of data classes such as Procedures, Orders, Problems, Diagnostic Imaging, and Laboratory, where anatomical specificity is frequently necessary for accurate understanding and exchange. Draft USCDI v7 already emphasizes contextual information and clearer implementation guidance, and anatomic localization fits naturally within that direction.
Thank you again for the opportunity to provide feedback. We appreciate ASTP/ONC's work in developing USCDI and would welcome continued engagement on how standardized anatomic localization can support nationwide interoperability.
Submitted by nancywspector on
WEDI Comments on Draft USCDI v7
The Workgroup for Electronic Data Interchange (WEDI) is pleased to comment on the Draft U.S. Core Data for Interoperability Version 7 (Draft USCDI v7) released by the Office of the National Coordinator for Health Information Technology (ONC) through Standards Bulletin 2026-1 on January 29, 2026.
WEDI was formed in 1991 by then Department of Health and Human Services (HHS) Secretary Dr. Louis Sullivan to identify opportunities to improve the efficiency of health data exchange. Named in the Health Insurance Portability and Accountability Act as an advisor to the Secretary of HHS, WEDI is the leading multi-stakeholder authority on the use of health information technology (IT) to efficiently improve health information exchange, enhance care quality, and reduce costs. With a focus on advancing standards for electronic administrative transactions, and promoting data privacy and security, WEDI is recognized and trusted as a formal advisor to the Secretary. Our diverse membership includes health plans, providers, standards development organizations, vendors, federal and state government agencies, and patient advocacy organizations.
WEDI is aware that Draft USCDI v7 continues ONC’s ongoing commitment to expanding standardized health data exchange to support improved patient care, improved data interoperability, and reduced clinician burden. Draft USCDI v7 proposes a total of 30 new and revised data elements across multiple data classes and we understand that these proposals were informed by extensive stakeholder feedback.
WEDI submits the following comments focused on areas where USCDI v7 proposals intersect most directly with WEDI’s work and where clarifications can improve implementation and reduce burden, as well as general comments on USCDI:
• WEDI supports:
o The continued evolution of USCDI as a “floor” for interoperable exchange and recognizes ONC’s emphasis on predictable, transparent updates.
o Draft USCDI v7’s overall direction, including proposed additions that address administrative burden reduction, care coordination, and data attributes.
o Expanding the guidance on scope clarity and “code system examples” where ambiguity could lead to inconsistent data capture and exchange.
• ONC should emphasize:
o Harmonization with administrative transactions and application programming interfaces (APIs) where USCDI intersects with eligibility and benefits, referrals, and prior authorization to avoid parallel, inconsistent approaches.
o Governance and freshness for dynamic data elements where the exchange value depends on clear expectations for data provenance, refresh frequency, and source of truth.
• ONC should re-evaluate the need for the proposed new data elements for Health Insurance Information, as they may cause confusion between data collected and shared through USCDI vs. administrative transactions that are likely more accurate. Confusion about the data elements Health Insurance Payer, Health Insurance Plan, and Health Insurance Plan Identifier will likely lead to use of free text or local codes, providing limited benefits for interoperability. Additionally, guidance on how “as of” dates and source attribution should be conveyed will be necessary, along with clarification on which data elements can support workflows but not replace administrative functions (eligibility and benefits verification) as these data elements are integral to administrative simplification but risk real-world usability if used inconsistently.
• Specific to the data classes, ONC should provide additional details on:
o Appointment by clarifying minimum data expectations and encouraging consistent workflows, as scheduling is foundational to operational interoperability and patient access, but “appointment” can be implemented inconsistently without clear guidance.
o Referral Order and Referral Note:
by clarifying how they connect to Appointment, Encounter, and the receiving organization; providing guidance and examples for “referral request” vs. “consult request” vs. “transition of care” communications to reduce inconsistent implementations
by encouraging alignment with API-based coordination workflows so referral content can be used downstream, as referrals are a major friction point across providers and payers
o Reason Not Performed:
by providing structured category guidance and examples to prevent implementers from using text-based, narrative reasons
by adding a burden-reduction note encouraging reuse of existing workflow artifacts instead of requiring new documentation
by clarifying association rules to link to the specific intended activity, as this data element has strong potential to reduce administrative churn but only if captured in a consistent and computable manner
o Diagnostic Imaging Reference:
by adding guidance on the minimum metadata needed for safe retrieval and matching (study identifiers, modality, performing organization, acquisition date/time, patient matching hints)
by adding guidance on secure access patterns appropriate for patient-facing and provider-facing use cases
by aligning with parallel federal workstreams addressing imaging interoperability (to support, rather than fragment, the emerging approach), as image retrieval across organizations is a persistent administrative burden
o Patient Identifier by clarifying the types of patient identifiers being considered and how they should be represented to prevent confusion with other identifiers and inappropriate reuse outside intended contexts, as patient matching remains a pervasive operational issue.
• In moving forward with expanding the USCDI and removing certification criteria in the ONC Health IT Certification Program, as proposed in the “Health Data, Technology, and Interoperability: ASTP/ONC Deregulatory Actions to Unleash Prosperity” (HTI-5), ONC should consider:
o How USCDI stays tightly defined as a minimum dataset
o Transparent criteria and review process used to move data elements or data classes from USCDI+ into USCDI
o Representation of USCDI elements in FHIR resources
o Potential for shifting burden and complexity from one stakeholder to another as USCDI expands but certification guardrails decrease, particularly in the context of overlapping implementation timelines and varying organizational readiness
o Potential for USCDI to support other administrative simplification needs, such as claims attachments data content
WEDI supports ONC’s work in developing a standardized minimum data set to be implemented across the health care ecosystem driving interoperability by keeping pace with clinical, technology, and policy changes. We believe several proposed additions to USCDI v7 (particularly Appointment, Referral Order/Note, Reason Not Performed, Diagnostic Imaging Reference, and Patient Identifier) could materially reduce administrative burden and improve interoperability with the additions outlined above.
We appreciate the opportunity to share our perspective on the Draft USCDI v7. We hope our comments will serve to assist ONC as it moves forward with these proposals. Please contact Robert Tennant, WEDI Executive Director, at rtennant@WEDI.org with any questions on these comments.
Help
1. Optional: Background Text / Cover Letter
The "Optional Background Text / Cover Letter" field provides space for additional context or introductory information related to your comment.
If you wish to provide context, explanation, or an introduction to your comment, enter this information in the field labeled "Optional Background Text / Cover Letter." This is entirely optional and is most useful when submitting multiple related comments or when additional background would help reviewers understand your feedback.
If you are only commenting on a single data class or element, you may leave this field blank.
2. Select the Data Class
To specify which data class your comment addresses:
- In the "Data Class" drop-down menu, select the appropriate data class you want to comment on.
- If you are providing a general comment that is not specific to a data element, select "General" from the options. Comments with this designation will be displayed on the USCDI landing page.
- Note that the Data Class field will automatically populate based on your current location in the platform:
- If you are on a data class page, the field will be set to that specific data class
- If you are on a data element page, the corresponding data class will be pre-selected
3. Select the Data Element
To specify which data element your comment addresses:
- In the "Data Element" drop-down menu, select the specific data element you want to comment on.
- The drop-down menu will display only the elements available under the data class you selected in the previous step.
- You can use the search function within the drop-down to quickly locate a specific data element.
- If you are commenting on the data class itself rather than a specific element, you may leave this field blank.
Note: Comments on a specific data element will appear on the respective data element page, while comments on a data class (without a specific element selected) will appear on the landing page for that data class.
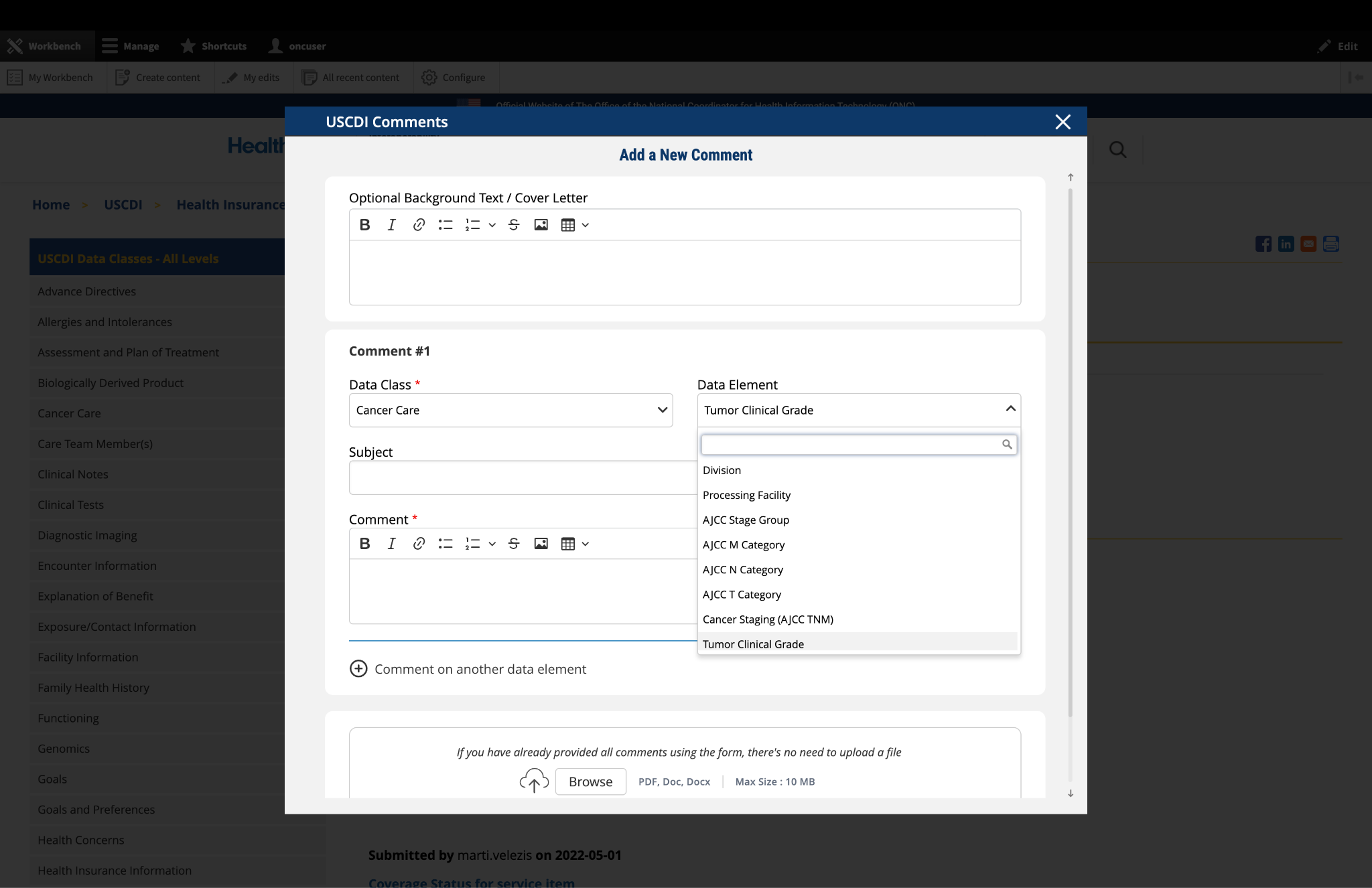
Fig 1 The "Data Class" and "Data Element" dropdown menus allow users to specify the exact content they wish to comment on.
4. Optional: Propose New Data Class or Element
If you cannot find the appropriate data class or element for your comment:
- Instead of clicking the "Comment On An Existing Data Class Or Element" button, click the adjacent button labeled "Propose a New Data Class or Data Element."
- This will redirect you to the ONDEC (ONC New Data Element and Class) Submission System.
- In the ONDEC system, follow the provided instructions to submit your proposal for a new data class or element.
- Once your proposal is submitted through ONDEC, it will be reviewed separately from the commenting process.
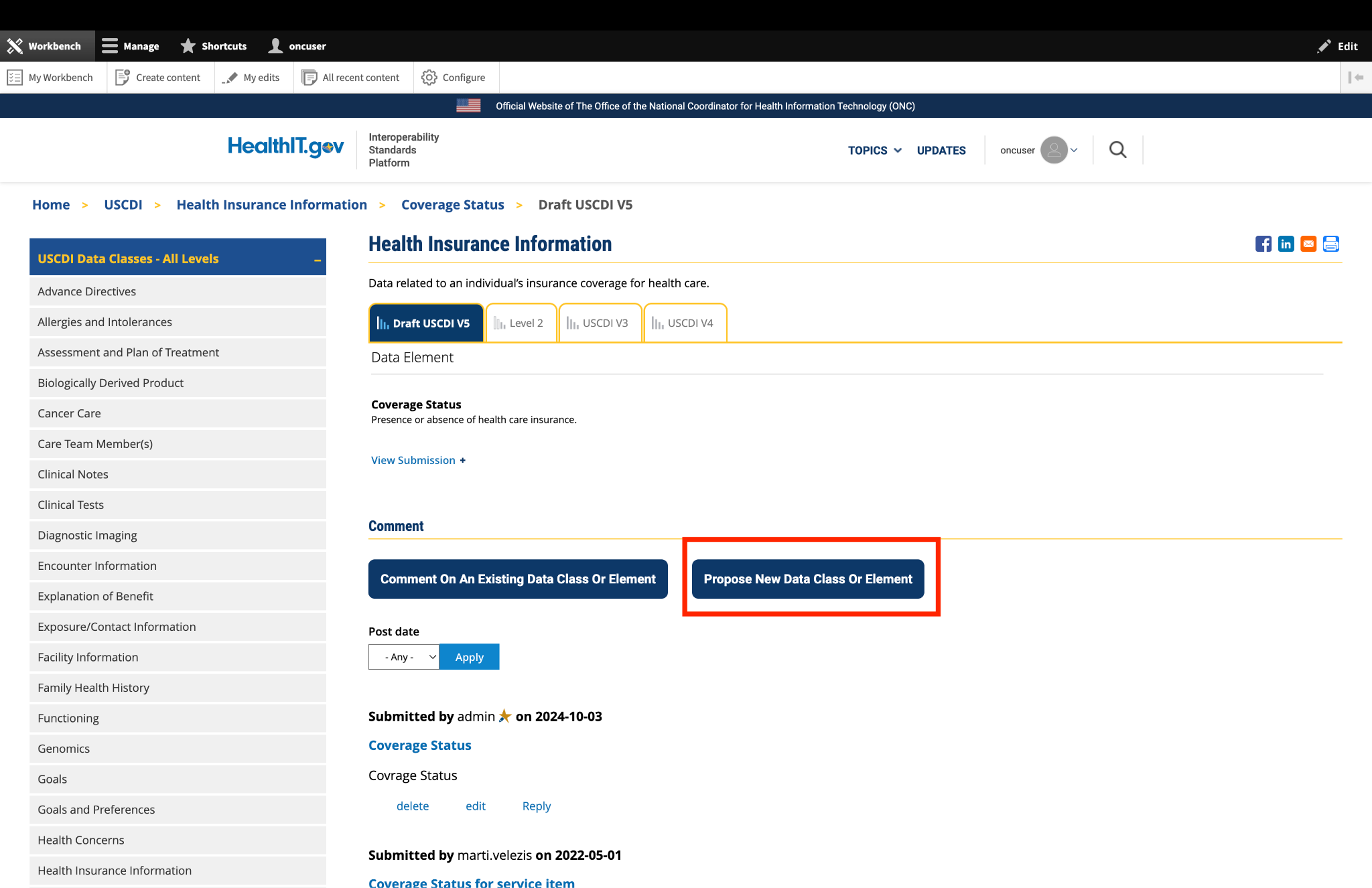
Fig 2 The "Propose a New Data Class or Data Element" button redirects users to the ONDEC Submission System for proposing new data elements not currently available in the system.
5. Complete the Comment Form
Fill out the required fields in the comment form:
Subject: Enter a brief, descriptive title that summarizes your comment. This helps reviewers quickly understand the nature of your feedback.
Comment: In this field, provide the full details of your comment or feedback. Be as clear and specific as possible about your suggestions, concerns, or observations. Include any relevant details that support your position.
6. Optional: Add Additional Comments
If you need to comment on multiple data classes or elements:
- After completing your first comment, click the link labeled "Comment on another data element" at the bottom of the form.
- A new comment section will appear, allowing you to enter details for your additional comment.
- For each additional comment, you must select the appropriate data class and data element from the drop-down menus.
- Complete the Subject and Comment fields for your additional comment.
- Repeat this process for each additional comment you wish to submit.
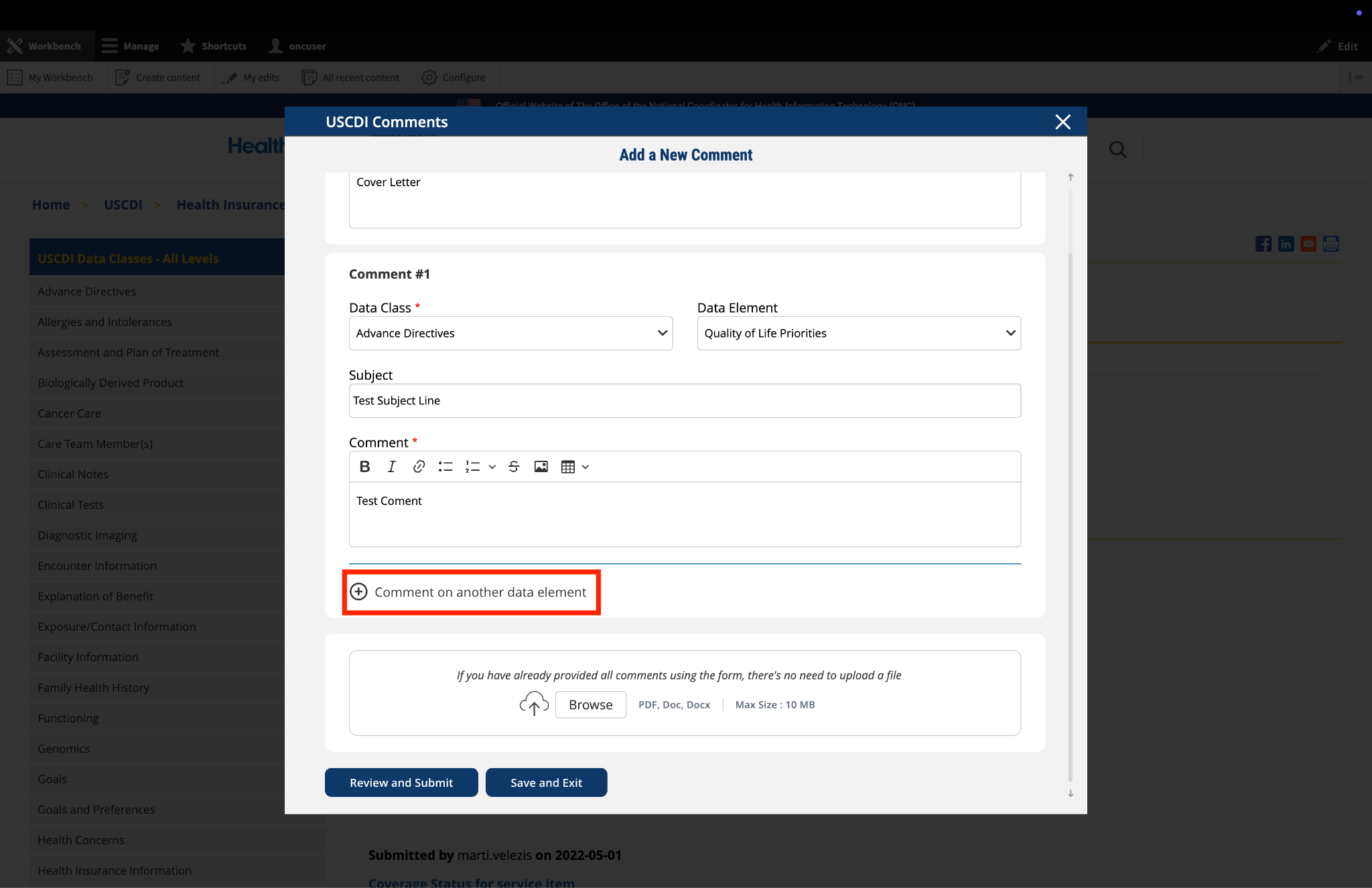
Fig 3 The "Comment on another data element" link enables users to create multiple comments addressing different elements within a single submission.
7. Optional: Upload Supporting Files
The platform allows you to upload supporting documentation to enhance your comment:
- Locate the "File Upload" section at the bottom of the comment form.
- Click to upload any files (such as PDFs or documents) that provide additional context, evidence, or clarification for your comment.
Important: If you have already entered your comments using the form fields, there is no need to upload duplicate content in PDF format. The file upload feature is intended for supplementary materials only. Please avoid uploading files that contain the same information already provided in your comment text.
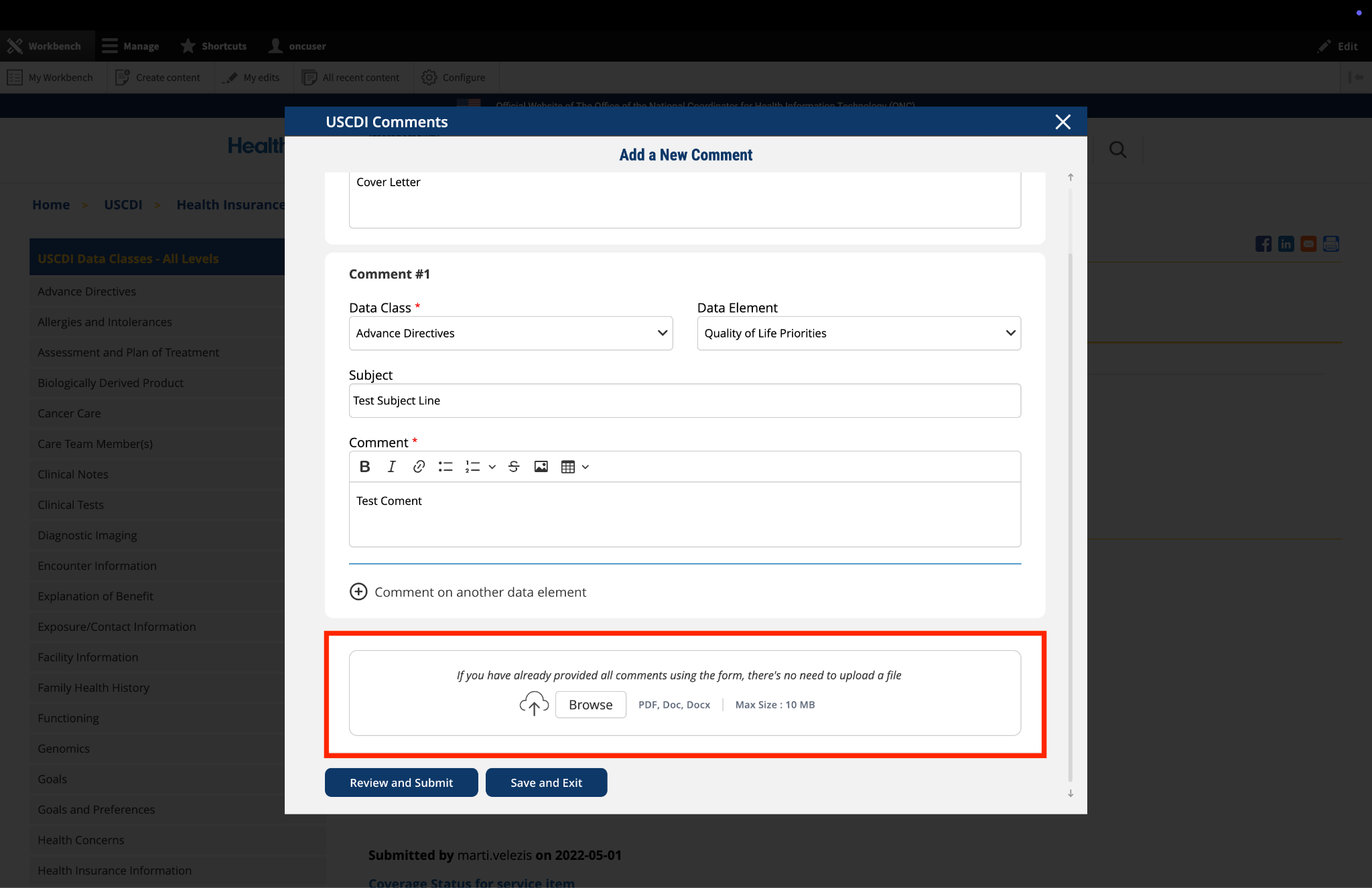
Fig 4 The "File Upload" section permits users to attach supporting documentation that supplements their written comments.
8. Optional: Save and Exit
If you need to pause your work and return to complete your comment later:
- Click the "Save and Exit" button at the bottom of the form.
- Your comment will be saved as a draft that you can access and complete later.
- When you return to the platform, you will see a red triangle with an exclamation mark next to the “Return to saved Comment” button, indicating that you have saved comments in draft status.
- Click this button to continue working on your draft.
- You will be taken to a review page where you can:
- Select "Submit Comment" to officially submit your feedback.
- Click "Edit" to return to the comment form and make changes
- Select "Discard Draft" to delete the saved draft and start fresh
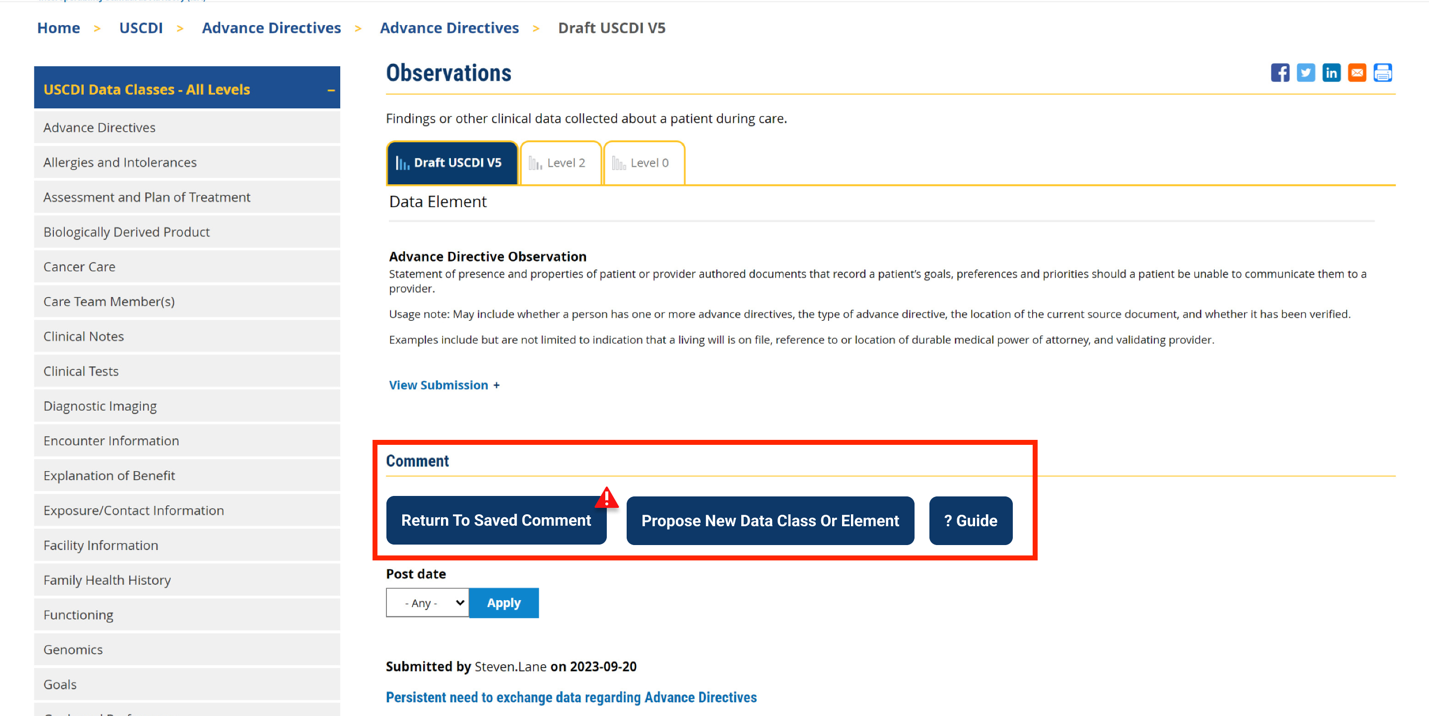
Fig 5 A red triangle with exclamation mark indicator appears next to the “Return to saved Comment” button when draft comments are saved in the system.
9. Review and Submit
Once you have completed your comment:
- Click the "Review and Submit" button at the bottom of the form.
- This will take you to a review screen displaying your comment(s) in full.
- Review all information for accuracy and completeness.
- On this review screen, you have three options:
- Click "Submit Comment" to officially submit your feedback
- Click "Edit" to return to the comment form and make changes
- Click "Discard Draft" to delete the comment and start fresh
- The review screen also includes a "Print" button that allows you to create a printed copy of your comments for your records.
- If you choose to submit, your comment will be recorded in the system and made available for review by the appropriate stakeholders.
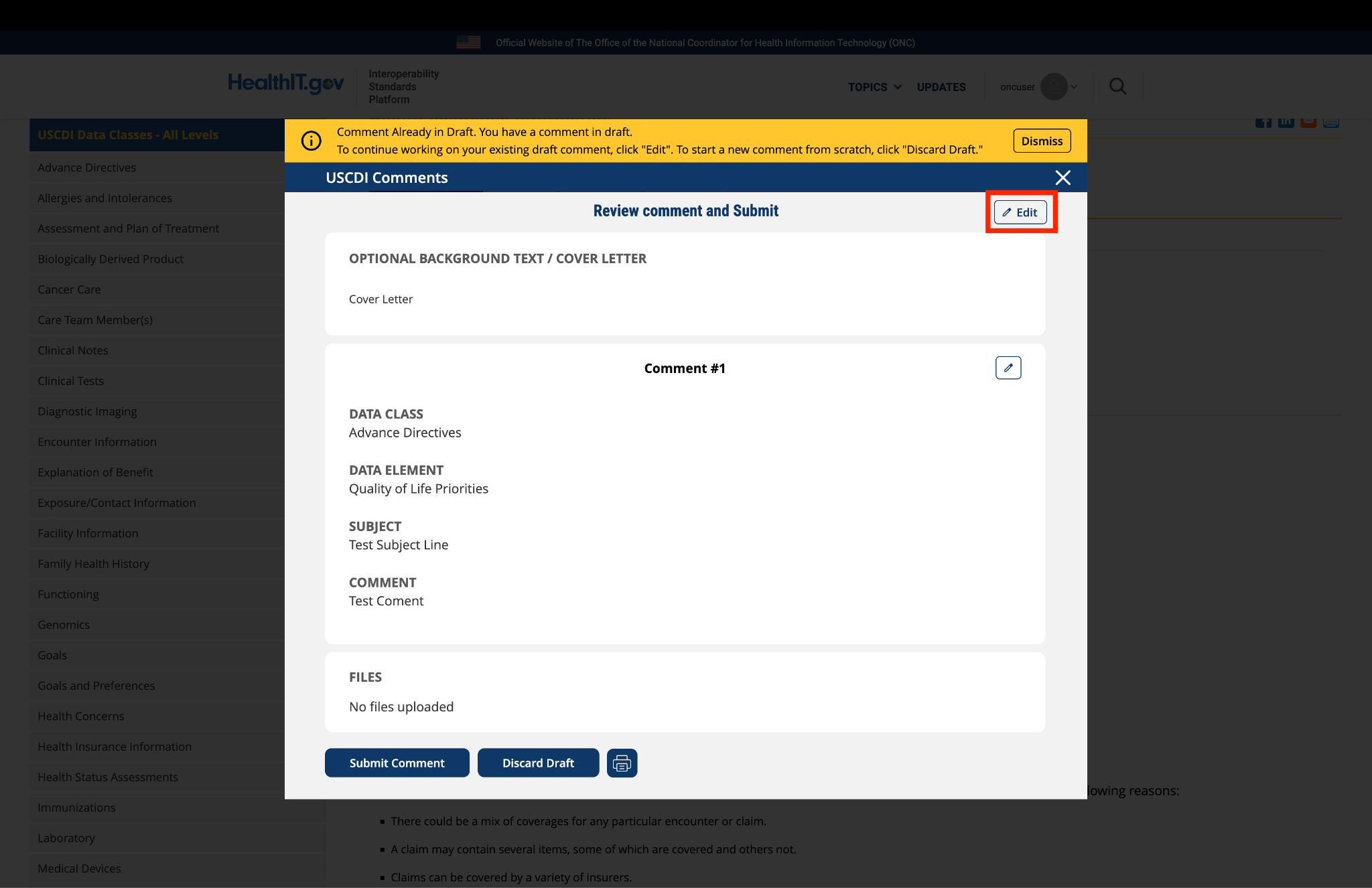
Fig 6 The review screen allows users to verify comment content and make any necessary modifications before final submission.
Submitted by cgutierrez@med… on
MEDITECH Comments on USCDI Draft v7
Medical Information Technology, Inc. (MEDITECH) is pleased to offer comments on the United States Core Data for Interoperability (USCDI) Draft Version 7. Please see attached document.
MEDITECH USCDI v7 Comments.pdf