
United States Core Data for Interoperability (USCDI)
The United States Core Data for Interoperability (USCDI) is a standardized set of health data classes and constituent data elements for nationwide, interoperable health information exchange. Review the USCDI Fact Sheet to learn more.
A USCDI Data Class is an aggregation of Data Elements by a common theme or use case.
A USCDI Data Element is a piece of data defined in USCDI for access, exchange or use of electronic health information.
USCDI ONC New Data Element & Class (ONDEC) Submission System
- USCDI V1
- USCDI V2
- USCDI V3
- USCDI V3.1
- USCDI V4
- USCDI V5
- USCDI V6
- Draft USCDI V7
- Level 2
- Level 1
- Level 0
USCDI V1
Please reference the USCDI version 1 document to the left for applicable standards versions associated with USCDI v1.
Harmful or undesired physiological responses associated with exposure to a substance.
Health professional’s conclusions and working assumptions that will guide treatment of the patient.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Desired state to be achieved by a patient.
Health related matter that is of interest, importance, or worry to someone who may be the patient, patient’s family or patient’s health care provider.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Representing a patient’s smoking behavior.
Unique identifier(s) for a patient's implantable device(s).
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V2
The USCDI v2 contains data classes and elements from USCDI v1 and new data classes and elements submitted through the ONDEC system. Please reference the USCDI Version 2 document to the left for applicable vocabulary standards versions associated with USCDI v2 and to the ONC Standards Bulletin 21-3 for more information about the process to develop USCDI v2 and future versions.
Harmful or undesired physiological responses associated with exposure to a substance.
Health professional’s conclusions and working assumptions that will guide treatment of the patient.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Desired state to be achieved by a patient.
Health related matter that is of interest, importance, or worry to someone who may be the patient, patient’s family or patient’s health care provider.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Representing a patient’s smoking behavior.
Unique identifier(s) for a patient's implantable device(s).
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V3
Please read the USCDI v3 standard document and the ONC Standards Bulletin 22-2 for details. Consistent with EO 14168 and OPM guidance, ASTP/ONC is exercising enforcement and issuing certification guidance for the ONC Health IT Certification Program with respect to certain data elements in USCDI v3. For more information see https://www.healthit.gov/topic/uscdi-v3-data-elements-enforcement-discretion.
Harmful or undesired physiological responses associated with exposure to a substance.
Health professional’s conclusions and working assumptions that will guide treatment of the patient.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Desired state to be achieved by a patient.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Unique identifier(s) for a patient's implantable device(s).
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V3.1
Please read the USCDI v3.1 standard document and the ONC Standards Bulletin 22-2 for details. USCDI version 3.1 updates USCDI version 3 with the following changes: consistent with Executive Order 14168, the Sex, Sexual Orientation, and Gender Identity data elements have been removed or updated in the Patient Demographics/Information Data Class.
Harmful or undesired physiological responses associated with exposure to a substance.
Health professional’s conclusions and working assumptions that will guide treatment of the patient.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Desired state to be achieved by a patient.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Unique identifier(s) for a patient's implantable device(s).
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V4
USCDI v4 added 20 data elements and one data class to USCDI v3. Please reference the USCDI v4 standard document and the ONC Standards Bulletin 23-2 for details. To review the prioritization criteria ONC used to select the USCDI v4 data elements, refer to the ONC Standards Bulletin 22-2.
Harmful or undesired physiological responses associated with exposure to a substance.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Physical place of available services or resources.
Desired state to be achieved by a person or a person’s elections to guide care.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
Information that guides treatment of the patient and recommendations for future treatment.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V5
USCDI v5 was published on July 16, 2024, and includes 16 new data elements and two new data classes. Please read the USCDI v5 standard document and the ONC Standards Bulletin 24-2 for details.
Harmful or undesired physiological responses associated with exposure to a substance.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Physical place of available services or resources.
Desired state to be achieved by a person or a person’s elections to guide care.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Findings or other clinical data collected about a patient during care.
Provider-authored request for the delivery of patient care services.
Usage notes: Orders convey a provider’s intent to have a service performed on or for a patient, or to give instructions on future care.
Data used to categorize individuals for identification, records matching, and other purposes.
Information that guides treatment of the patient and recommendations for future treatment.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
USCDI V6
ASTP/ONC published USCDI v6 on July 24, 2025, which includes 6 new data elements. Please read the USCDI v6 Standard Document and the ASTP/ONC Standards Bulletin 25-2 for details. ASTP/ONC welcomes input on future versions during the USCDI feedback period, open through September 29, 2025, at 11:59 PM ET. During this time, ASTP/ONC is accepting new data element submissions through ONDEC, and comments on existing data elements may be entered via the updated commenting feature on the USCDI data element pages.
Harmful or undesired physiological responses associated with exposure to a substance.
Information that guides treatment of the patient and recommendations for future treatment.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Physical place of available services or resources.
Family member health condition(s) that are relevant to a patient's care.
Desired state to be achieved by a person or a person’s elections to guide care.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Provider-authored request for the delivery of patient care services.
Usage notes: Orders convey a provider’s intent to have a service performed on or for a patient, or to give instructions on future care.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
Draft USCDI V7
ASTP/ONC published Draft USCDI v7 on January 29, 2026, which includes 30 new data elements. For the official reference, please read the Draft USCDI v7 Standards Document; the ASTP/ONC Standards Bulletin 26-1 provides additional information. ASTP/ONC welcomes input on future versions during the USCDI feedback period, open through April 13, at 11:59 PM ET. During this time, ASTP/ONC is accepting new data element submissions through ONDEC, and comments on data elements may be entered via the updated commenting feature on the USCDI data element pages.
Unintended effects associated with clinical interventions.
Harmful or undesired physiological responses associated with exposure to a substance.
Information that guides treatment of the patient and recommendations for future treatment.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Physical place of available services or resources.
Family member health condition(s) that are relevant to a patient's care.
Desired state to be achieved by a person or a person’s elections to guide care.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Contextual information that provides supporting details for healthcare data.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Provider-authored request for the delivery of patient care services.
Usage notes: Orders convey a provider’s intent to have a service performed on or for a patient, or to give instructions on future care.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
- Represented by a terminology standard or SDO-balloted technical specification or implementation guide.
- Data element is captured, stored, or accessed in multiple production EHRs or other HIT modules from more than one developer.
- Data element is electronically exchanged between more than two production EHRs or other HIT modules of different developers using available interoperability standards.
- Use cases apply to most care settings or specialties.
Level 2
Unintended effects associated with clinical interventions.
Harmful or undesired physiological responses associated with exposure to a substance.
Material substance originating from a biological entity intended to be transplanted or infused into another (possibly the same) biological entity.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Physical place of available services or resources.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Contextual information that provides supporting details for healthcare data.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Provider-authored request for the delivery of patient care services.
Usage notes: Orders convey a provider’s intent to have a service performed on or for a patient, or to give instructions on future care.
Data used to categorize individuals for identification, records matching, and other purposes.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
- Represented by a terminology standard or SDO-balloted technical specification or implementation guide.
- Data element is captured, stored, or accessed in at least one production EHR or HIT module.
- Data element is electronically exchanged between two production EHRs or other HIT modules using available interoperability standards.
- Use cases apply to several care settings or specialties.
Level 1
Material substance originating from a biological entity intended to be transplanted or infused into another (possibly the same) biological entity.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Physical place of available services or resources.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Analysis of clinical specimens to obtain information about the health of a patient.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Data used to categorize individuals for identification, records matching, and other purposes.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.
- Not represented by a terminology standard or SDO-balloted technical specification or implementation guide.
- Data element is captured, stored, or accessed in limited settings such as a pilot or proof of concept demonstration.
- Data element is electronically exchanged in limited environments, such as connectathons or pilots.
- Use cases apply to a limited number of care settings or specialties, or data element represents a specialization of other, more general data elements.
Level 0
Unintended effects associated with clinical interventions.
Harmful or undesired physiological responses associated with exposure to a substance.
Material substance originating from a biological entity intended to be transplanted or infused into another (possibly the same) biological entity.
Information about a person who participates or is expected to participate in the care of a patient.
Narrative patient data relevant to the context identified by note types.
-
- Usage note: Clinical Notes data elements are content exchange standard agnostic. They should not be interpreted or associated with the structured document templates that may share the same name.
Non-imaging and non-laboratory tests performed that result in structured or unstructured findings specific to the patient to facilitate the diagnosis and management of conditions.
Tests that result in visual images requiring interpretation by a credentialed professional.
Information related to interactions between healthcare providers and a patient.
Health data as reflected in a patient's Explanation of Benefits (EOB) statements, typically derived from claims and other administrative data.
Physical place of available services or resources.
Desired state to be achieved by a patient.
Desired state to be achieved by a person or a person’s elections to guide care.
Data related to an individual’s insurance coverage for healthcare.
Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s authorized representative, or patient’s healthcare provider that could identify a need, problem, or condition.
Record of vaccine administration.
Analysis of clinical specimens to obtain information about the health of a patient.
Instrument, machine, appliance, implant, software, or similar device intended to be used for a medical purpose.
Pharmacologic agents used in the diagnosis, cure, mitigation, treatment, or prevention of disease.
Findings or other clinical data collected about a patient during care.
Provider-authored request for the delivery of patient care services.
Usage notes: Orders convey a provider’s intent to have a service performed on or for a patient, or to give instructions on future care.
Data used to categorize individuals for identification, records matching, and other purposes.
Information that guides treatment of the patient and recommendations for future treatment.
Condition, diagnosis, or reason for seeking medical attention.
Activity performed for or on a patient as part of the provision of care.
The metadata, or extra information about data, regarding who created the data and when it was created.
Physiologic measurements of a patient that indicate the status of the body’s life sustaining functions.


The USCDI ONC New Data Element and Class (ONDEC) Submission System supports a predictable, transparent, and collaborative process, allowing health IT stakeholders to submit new data elements and classes for future versions of USCDI. Click here for more information and to submit new data elements.
The USCDI standard will follow the Standards Version Advancement Process described in the Cures rule to allow health IT developers to update their systems to newer version of USCDI and provide these updates to their customers.
Comment
Submitted by sdeplonty on
Pathology reports
This field is for general comments on the USCDI. I think you should reconsider having Pathology reports as part of this data set. One part of the elements says that it should be easily read and understood, neither of which a pathology report is. I know version two is just moving them from clinical notes to their own pathology category, but I feel these are reports that can cause a patient to panic and then maybe not be able to get into their provider right away. Please reconsider these being part of the set.
Thank you.
Submitted by LisaRNelson on
Do you intend the USCDI to support a multiaxial heirarchy?
If you make Orders a Data Class, then you need to decide if you will allow notions to be categorized in more than one place or not. For example, orders for laboratory, pathology, and diagnostic imaging tests, should those data elements be covered in those respective data classes, or should those data elements be shown within the Orders data class? Or should they show in both places?Submitted by LisaRNelson on
Do you intend the USCDI to support a multiaxial heirarchy?
If you make Orders a Data Class, then you need to decide if you will allow notions to be categorized in more than one place or not. For example, orders for laboratory, pathology, and diagnostic imaging tests, should those data elements be covered in those respective data classes, or should those data elements be shown within the Orders data class? Or should they show in both places?Submitted by LisaRNelson on
Do you intend the USCDI to support a multiaxial heirarchy?
If you make Orders a Data Class, then you need to decide if you will allow notions to be categorized in more than one place or not. For example, orders for laboratory, pathology, and diagnostic imaging tests, should those data elements be covered in those respective data classes, or should those data elements be shown within the Orders data class? Or should they show in both places?Submitted by LisaRNelson on
Referral Data Class
The Referral Data Class is much more mature than this Comment level characterizes. The Referral Note document type has been recommended for Certified EHR Technology along with CCD and Discharge Summary since Meaningful Use Stage 1. Further more, the IHE 360X Profile has been demonstrating it's use of multiple years at HIMSS Show Case demonstrations and other ONC, IHE and DirectTrust events. This March at the IHE Connectathon three well known EHRs and one HIE solution vendor successfully tested/demonstrated their support of the 360X profile and they were generating Referral Note documents containing all the proposed data elements within:
Referral Coverage information in really "insurance information" typically categorized as "Payer Information" in the C-CDA paradigm. This data element faces challenges because to date there is not a national identification system to indicate what health plan is providing the coverage. Until this larger problem gets solved, representing coverage information will be challenging.
Submitted by Terry Fulmer on
I've now review draft…
I've now review draft version two of the USCDI document you sent and thank you for the opportunity. My overall my main recommendation is that somewhere there needs to be a very clear indication of functional assessment. Function in terms of the ability to do ADLs and IADLs and what we, with IHI refer to as the 4M assessment of age friendly health systems which includes “what matters mentation medication and mobility. The opportunity to have interoperability is critical and this work is vital. I am always concerned when we focus on conditions instead of the capacity a person has within the context of conditions. Lots of people have heart failure and some are playing tennis while others are lying in bed.
So functional assessment.
Submitted by Terry Fulmer on
This field is for general…
I've now review draft version two of the USCDI document you sent and thank you for the opportunity. My overall my main recommendation is that somewhere there needs to be a very clear indication of functional assessment. Function in terms of the ability to do ADLs and IADLs and what we, with IHI refer to as the 4M assessment of age friendly health systems which includes “what matters mentation medication and mobility. The opportunity to have interoperability is critical and this work is vital. I am always concerned when we focus on conditions instead of the capacity a person has within the context of conditions. Lots of people have heart failure and some are playing tennis while others are lying in bed.
So functional assessment.
Submitted by sg999 on
CMS Comment on USCDI draft V2
On behalf of The Centers for Medicare and Medicaid Services (CMS) and The Center for Clinical Standards and Quality (CCSQ) we submit comment on the USCDI draft version 2, attached.
CMS supports a broader vision for the USCDI, where the USCDI standard serves as the central mechanism for exposing usable, standardized interoperable data for multiple use cases, including quality measurement. We are committed to working collaboratively with ONC to ensure the USCDI meets stakeholder needs. We specifically urge ONC to add additional data elements to USCDI version 2 that are critical for data sharing and addressing emerging public health needs as well as health equity, highlighted in the attached comment response.
Submitted by Grace Cordovano on
USCDI Draft v2: Comments from Patient & Carepartner Perspective
General Overview
- Based on the comments and feedback received to date on this entire body of work, what is the approximate percentage of responses by stakeholder category? For example, how much feedback and guidance has been received from vendors, payors, representatives from the government, clinicians, and actual patients, carepartners, and respective patient, non-profit advocacy groups? A simple pie chart would be helpful in defining this with more transparency. The suggestion, prioritization, and implementation of new data classes and data elements will be a direct consequence of the representation of stakeholders. If patients, carepartners, and advocates have not been well represented, the USCDI expansion will not be inclusive of diverse voices nor represent the unmet needs of patients and their families.
- When presenting USCDI draft versions for feedback from the public, v2 or future versions moving forward, it would be helpful, on pages 5-14, to see specific examples of how each respective data class and data element is represented using synthetic data.
- Disability status or need for accessibility support is not captured. Over 61 million (roughly 1 in 4) adults in the United States live with a disability. https://www.cdc.gov/ncbddd/disabilityandhealth/infographic-disability-impacts-all.html#:~:text=61%20million%20adults%20in%20the,is%20highest%20in%20the%20South. If we are going to improve the lives and care of individuals living with disabilities, we must prioritize capturing and sharing this data accordingly.
- Page 4: Does not list Data Class "Goals" and Data Element "Patient Goals"; page 8 does.
- Imaging and pathology are recognized as data elements. Where are surgical/operative reports/notes reflected?
- It is gravely concerning to see that critical end-of-life care information, such as Advance Directives, Do Not Resuscitate (DNR) orders, Physician Orders for Life-Sustaining Treatment (POLST), are not included in the USCDI draft v2. These are essential to be documented. Throughout the COVID-19 pandemic, we witnessed reports of potential needs to ration care due to surging numbers of COVID-19 positive patients. Many patients with life-altering, life-limiting conditions were strongly encouraged to have their end-of-life wishes documented as a precaution. Pandemic and beyond, it is unethical that end-of-life care information that has the power to actionably communicate an individual's wishes at their end of life not only does not appear in draft v2 but also is only prioritized at level 1. By not including end-of-life care information, such as Advance Directives, DNRs, and POLST, the draft document sends the message that USCDI is prioritizing vendor and billing priorities rather than data elements and data classes that have universal applicability to every human being and doing right by the patient.
- The element "Diagnostic Imaging Narrative" as a separate entity from "Diagnostic Imaging Report" is unclear and confusing. Diagnostic Imaging Reports often have "Impressions," "Findings," "Summary," or "Observations" noted and should be referred to as such for consistency when discussed in the USCDI work. Impressions, Findings, Summaries, and Observations should not be codified to enable extraction from an imaging report without other essential elements of the respective report as this is not only counterproductive but can cause harm to inpatient care. Elements
- There are 61 data elements in total listed in USCDI draft v2; 25 data elements (41%) have no applicable standards listed. Some of these elements are self-explanatory and straightforward, while others have more room for interpretation and are vague, such as Patient's Goals, Date of Resolution, Care Team Members. Applicable, available standards should be assigned, and any remaining vagueness directly addressed so as to avoid amplifying confusion on implementation. The following do not have standards listed as of yet:
- Assessment and Plan of Treatment
- Care Team Members
- Provider Name
- Provider Identifier
- Encounter Type
- Encounter Time
- Patient's Goals
- Health Concerns
- Values/Results
- Laboratory Report Narrative
- Pathology Report Narrative
- First Name
- Last Name
- Previous Name
- Middle Name
- Suffix
- Date of Birth
- Current Address
- Previous Address
- Phone Number Type
- Email Address
- Date of Diagnosis
- Date of Resolution
- Author Time Stamp
- Author Organization
Specific Feedback
Allergies & Intolerance: Many people are allergic to things that are not a medication that they can encounter in a clinical setting, such as latex. This won't have a medication name or drug class.
Assessment & Plan of Treatment: Is this only capturing the clinical treatment plan? Is this capturing social determinants of health (SDoH)? If a health professional is not aware of various prominent barriers a patient is living with, the clinical treatment plan that is documented will fully fail the patient. For example, prescribing an expensive infusion treatment that is not covered by a patient's insurance company may cause significant harm to the patient as treatment is not affordable or accessible. If this is not understood before the patient leaves the clinic, a patient may learn about the treatment being not covered and simply not come back to the clinic and give up. This leads to disease progression and exacerbation of symptoms with the potential for eventually needing emergency room care. By understanding what SDoH factors may negatively impact a clinical treatment plan, adjustments may be made proactively as well as connecting the patient to community support and financial assistance resources. Recommend building a framework to capture elements of social determinants of health (SDoH) for future draft versions for prioritization from level 2.
Care Team Members: Is this only capturing clinical care team members? To be progressive, we must capture and include a patient's primary carepartner, advocate, executor of their estate, personal representative, etc. as the majority of care, especially in the chronic, life-altering, life-limiting settings, happens outside of the four walls of medicine requiring the support of non-clinical care team members. The Care Team Members Data Class and Data Element need more detail in the USCDI draft v2 description on page 6 to clarify ambiguity.
Clinical Notes: Operative notes are critical to patient continuity of care and patient safety. It is important to emphasize that operative notes are one of the only pieces of information that alert patients and their carepartners to the fact that tissue and biological samples may have been harvested during surgery and have been submitted for pathology and/or laboratory analysis. Operative notes need to be included under Clinical Notes in draft v2.
Diagnostic Imaging Narrative: An Imaging Narrative should not be available to be extracted without all the accompanying essential components of the imaging report. The concept of an Imaging Narrative is also unclear. Data Elements should be reflective of the wording used in the real world. An Imaging Narrative is typically referred to as the Findings/Impressions/Summary section of the imaging report and should be referred to as such for consistency.
Immunizations: Essential public health safety, reporting, and information exchange throughout the pandemic & for post-pandemic public health monitoring.
- Date- Include in draft v2 to monitor COVID19 vaccination doses and potential boosters
- Type- Consider adding vaccine type (brand/manufacturer) to draft v2 as COVID-19 vaccines requiring at least two doses currently can not be mixed and matched until clinical trial data proves heterologous prime-boost is safe and effective.
Laboratory:
- Laboratory Report Narrative- It is unclear what exactly a laboratory narrative is. A Laboratory Narrative should not be available to be extracted without all the accompanying essential components of the laboratory report.
- Pathology Report Narrative- A Pathology Report Narrative should not be available to be extracted without all the accompanying essential components, such as the microscopic analysis and diagnosis, of the laboratory report.
- Units of Measure- Laboratory values/results must have units of measure included. Draft v2 should include units of measure if Values/Results do not include them.
- Autopsy Report- This is an essential piece of reporting to bring peace and closure to families grieving the loss of loved ones, as well as essential information for public health and scientific understanding of the COVID-19 pandemic. Draft v2 should include information from autopsy reports
Medications:
- Dose- This is critical for patient safety, prevention of medication errors, and continuity of care purposes. Draft v2 should include medication dose; add to USCDI v2
- Prescribed By- Medications often have the most variation and inconsistency in documentation as prescriptions are frequently discontinued for numerous reasons. Patients may have 20+ medications in their medication history but may only be actively currently taking 2 or 3. There is currently no way to flag a medication as discontinued. Patients are frequently told by their care team that if they did not prescribe the medication, they could not delete or remove it from their medication list in the EHR. Medication corrections are a frequent reason for patients wanting to correct their medical records. Inaccurate medication lists upon patient intake, at patient discharge, and in pre-admission for surgery can be tedious/impossible for staff and patients to review and may endanger patient safety. Draft v2 should include information on who prescribed a medication; add to USCDI v2.
- Status- This is critical for patient safety, prevention of medication errors, and a frequent request for medical record addendums that would be of great importance to address proactively. Draft v2 should include information on whether a medication is active or discontinued. Add to USCDI v2
Problems: Date of Resolution is not broadly applicable to people living with chronic illness, life-altering, life-limiting conditions, disability, rare disease, terminal illness, and active death care and end-of-life. This is a vague data element that can bring great harm to patients should it be documented incorrectly or incompletely. The TF must be conscious of the potentially severe negative impact on patients' lives with respect to matters such as disability benefits should the data element be captured incorrectly or not comprehensively. Recommend removing from USCDI draft v2.
Procedures: Do surgical/operative reports/notes currently fall under this category?
Smoking Status: Tobacco Use more accurately describes the spectrum of individual behavior being captured in a less stigmatizing manner. TF should consider revising the data class and element name to "Tobacco Use".
Other:
- End of Life Care- End of Life Care is often intentionally distinct from routine care and should be reflected as such. Recommend adding "End of Life Care" as a distinct new data class.
- Advance Directive- Pandemic and beyond, it is unethical that end-of-life care information that has the power to actionably communicate an individual's wishes at their end of life not only does not appear in draft v2 but also is only prioritized at level 1. By not including end-of-life care information, such as Advance Directives, DNRs, and POLST, the draft document sends the message that USCDI is prioritizing vendor and billing priorities rather than data elements and data classes that have universal applicability to every human being and doing right by the patient. Recommend moving from L1 to draft v2.
- Blood Type- Blood type is an essential laboratory test that is often repetitively ordered throughout women's lives due to pregnancy and the lives of patients, such as those in need of a transfusion. It would be beneficial to capture this and reduce the need for repeat testing.
- Coverage Type- Due to the pandemic, millions of individuals have lost health coverage. In order to connect people to public resources as quickly as possible to ensure people have affordable, meaningful access to health care, information on Health Insurance Coverage Type must be prioritized.
Help
1. Optional: Background Text / Cover Letter
The "Optional Background Text / Cover Letter" field provides space for additional context or introductory information related to your comment.
If you wish to provide context, explanation, or an introduction to your comment, enter this information in the field labeled "Optional Background Text / Cover Letter." This is entirely optional and is most useful when submitting multiple related comments or when additional background would help reviewers understand your feedback.
If you are only commenting on a single data class or element, you may leave this field blank.
2. Select the Data Class
To specify which data class your comment addresses:
- In the "Data Class" drop-down menu, select the appropriate data class you want to comment on.
- If you are providing a general comment that is not specific to a data element, select "General" from the options. Comments with this designation will be displayed on the USCDI landing page.
- Note that the Data Class field will automatically populate based on your current location in the platform:
- If you are on a data class page, the field will be set to that specific data class
- If you are on a data element page, the corresponding data class will be pre-selected
3. Select the Data Element
To specify which data element your comment addresses:
- In the "Data Element" drop-down menu, select the specific data element you want to comment on.
- The drop-down menu will display only the elements available under the data class you selected in the previous step.
- You can use the search function within the drop-down to quickly locate a specific data element.
- If you are commenting on the data class itself rather than a specific element, you may leave this field blank.
Note: Comments on a specific data element will appear on the respective data element page, while comments on a data class (without a specific element selected) will appear on the landing page for that data class.
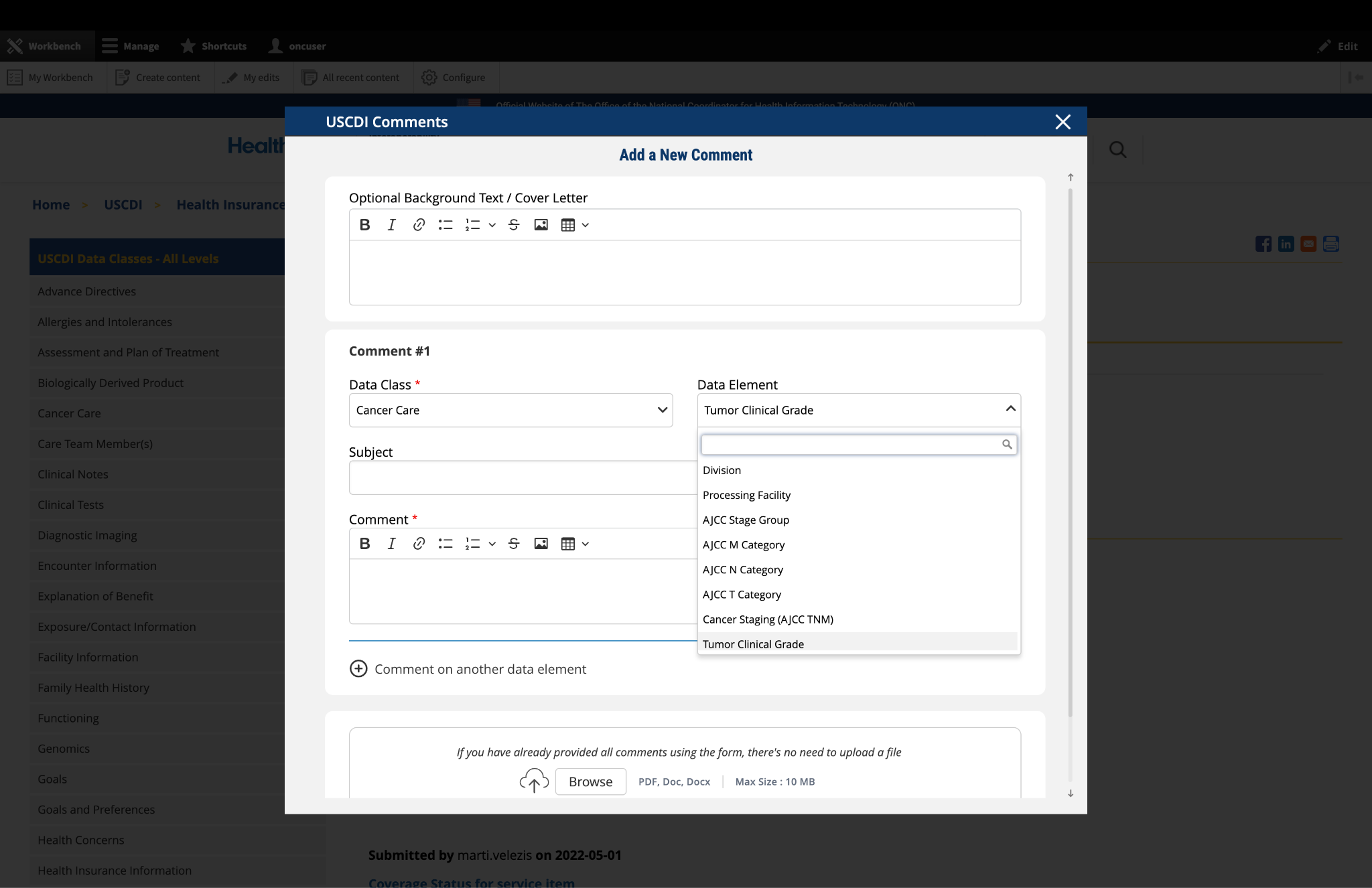
Fig 1 The "Data Class" and "Data Element" dropdown menus allow users to specify the exact content they wish to comment on.
4. Optional: Propose New Data Class or Element
If you cannot find the appropriate data class or element for your comment:
- Instead of clicking the "Comment On An Existing Data Class Or Element" button, click the adjacent button labeled "Propose a New Data Class or Data Element."
- This will redirect you to the ONDEC (ONC New Data Element and Class) Submission System.
- In the ONDEC system, follow the provided instructions to submit your proposal for a new data class or element.
- Once your proposal is submitted through ONDEC, it will be reviewed separately from the commenting process.
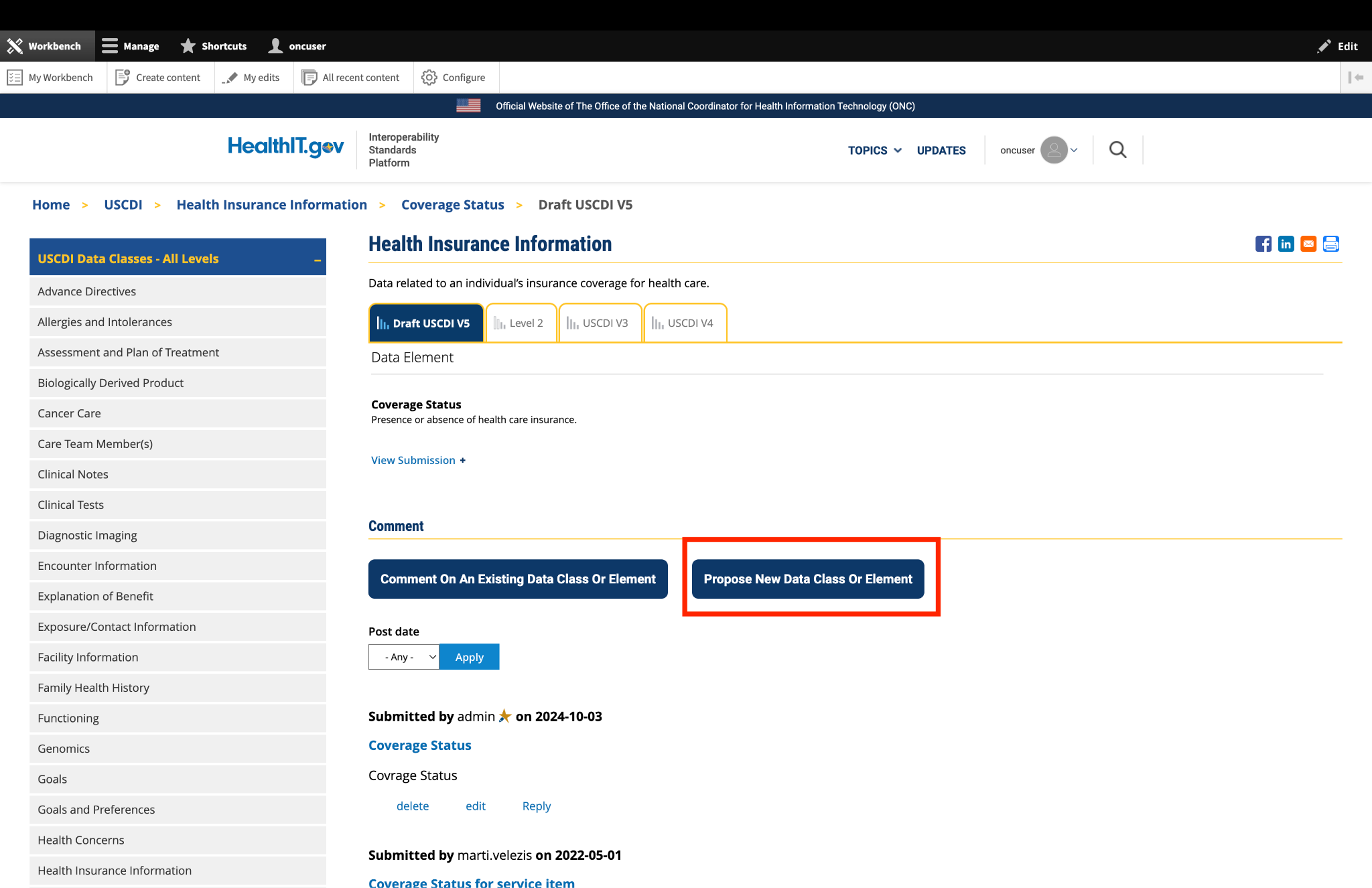
Fig 2 The "Propose a New Data Class or Data Element" button redirects users to the ONDEC Submission System for proposing new data elements not currently available in the system.
5. Complete the Comment Form
Fill out the required fields in the comment form:
Subject: Enter a brief, descriptive title that summarizes your comment. This helps reviewers quickly understand the nature of your feedback.
Comment: In this field, provide the full details of your comment or feedback. Be as clear and specific as possible about your suggestions, concerns, or observations. Include any relevant details that support your position.
6. Optional: Add Additional Comments
If you need to comment on multiple data classes or elements:
- After completing your first comment, click the link labeled "Comment on another data element" at the bottom of the form.
- A new comment section will appear, allowing you to enter details for your additional comment.
- For each additional comment, you must select the appropriate data class and data element from the drop-down menus.
- Complete the Subject and Comment fields for your additional comment.
- Repeat this process for each additional comment you wish to submit.
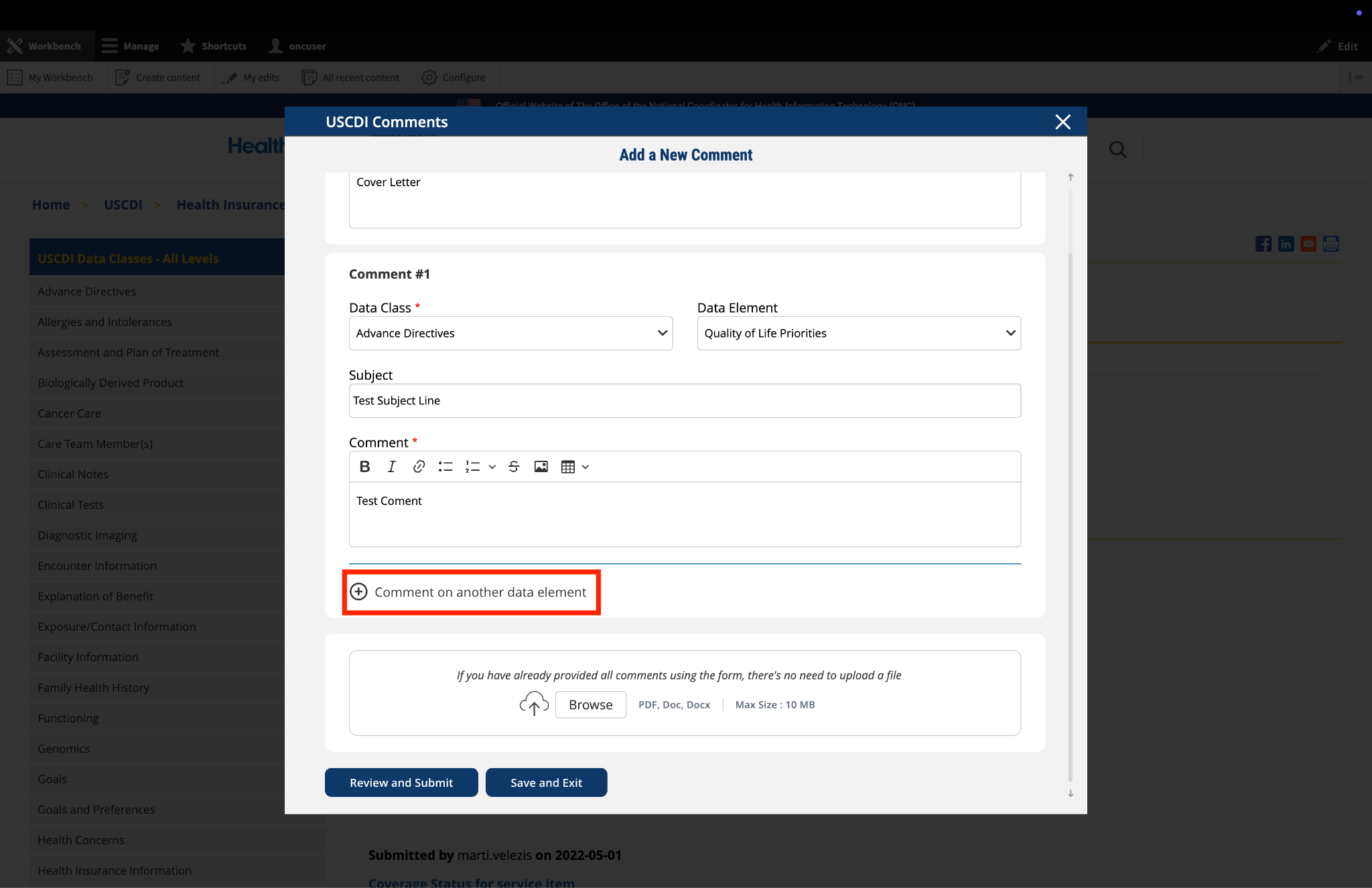
Fig 3 The "Comment on another data element" link enables users to create multiple comments addressing different elements within a single submission.
7. Optional: Upload Supporting Files
The platform allows you to upload supporting documentation to enhance your comment:
- Locate the "File Upload" section at the bottom of the comment form.
- Click to upload any files (such as PDFs or documents) that provide additional context, evidence, or clarification for your comment.
Important: If you have already entered your comments using the form fields, there is no need to upload duplicate content in PDF format. The file upload feature is intended for supplementary materials only. Please avoid uploading files that contain the same information already provided in your comment text.
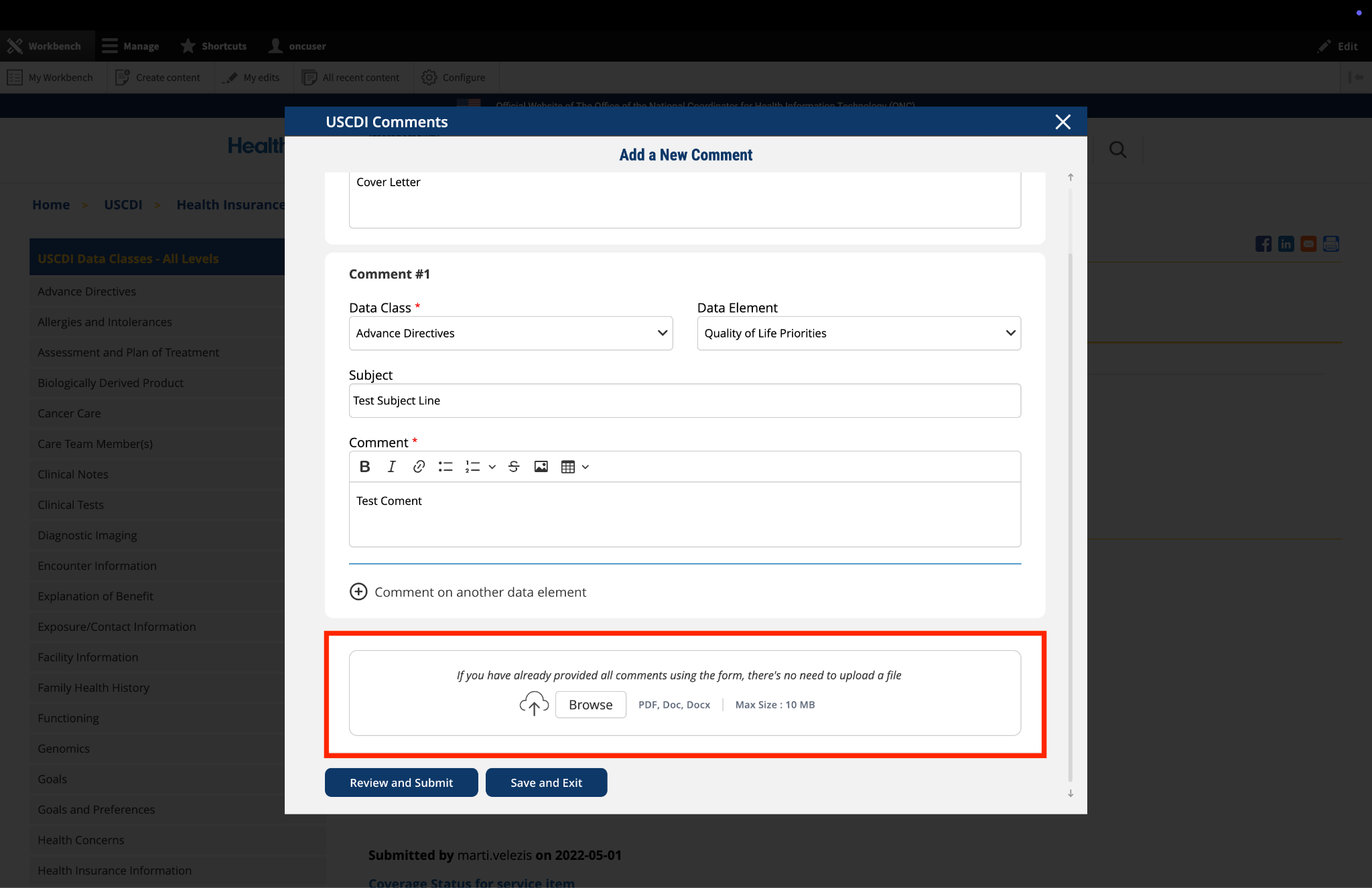
Fig 4 The "File Upload" section permits users to attach supporting documentation that supplements their written comments.
8. Optional: Save and Exit
If you need to pause your work and return to complete your comment later:
- Click the "Save and Exit" button at the bottom of the form.
- Your comment will be saved as a draft that you can access and complete later.
- When you return to the platform, you will see a red triangle with an exclamation mark next to the “Return to saved Comment” button, indicating that you have saved comments in draft status.
- Click this button to continue working on your draft.
- You will be taken to a review page where you can:
- Select "Submit Comment" to officially submit your feedback.
- Click "Edit" to return to the comment form and make changes
- Select "Discard Draft" to delete the saved draft and start fresh
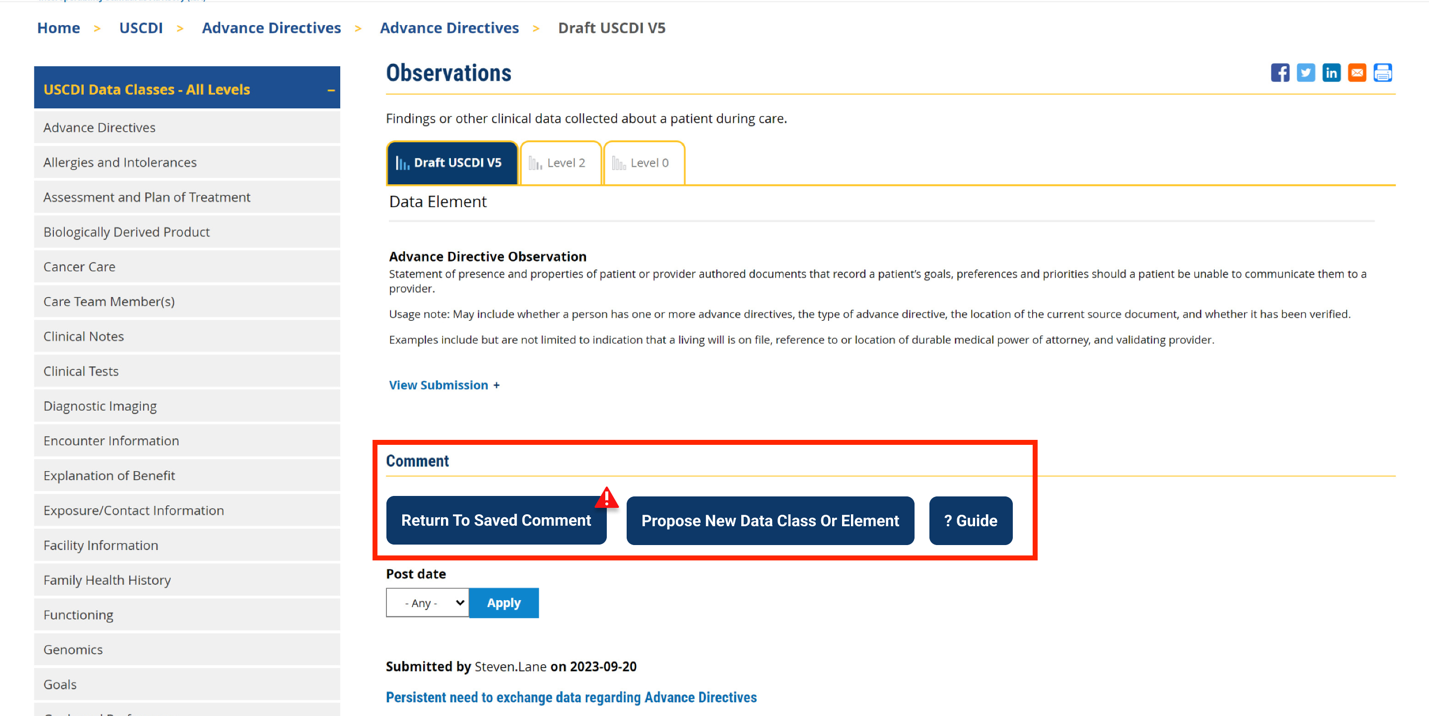
Fig 5 A red triangle with exclamation mark indicator appears next to the “Return to saved Comment” button when draft comments are saved in the system.
9. Review and Submit
Once you have completed your comment:
- Click the "Review and Submit" button at the bottom of the form.
- This will take you to a review screen displaying your comment(s) in full.
- Review all information for accuracy and completeness.
- On this review screen, you have three options:
- Click "Submit Comment" to officially submit your feedback
- Click "Edit" to return to the comment form and make changes
- Click "Discard Draft" to delete the comment and start fresh
- The review screen also includes a "Print" button that allows you to create a printed copy of your comments for your records.
- If you choose to submit, your comment will be recorded in the system and made available for review by the appropriate stakeholders.
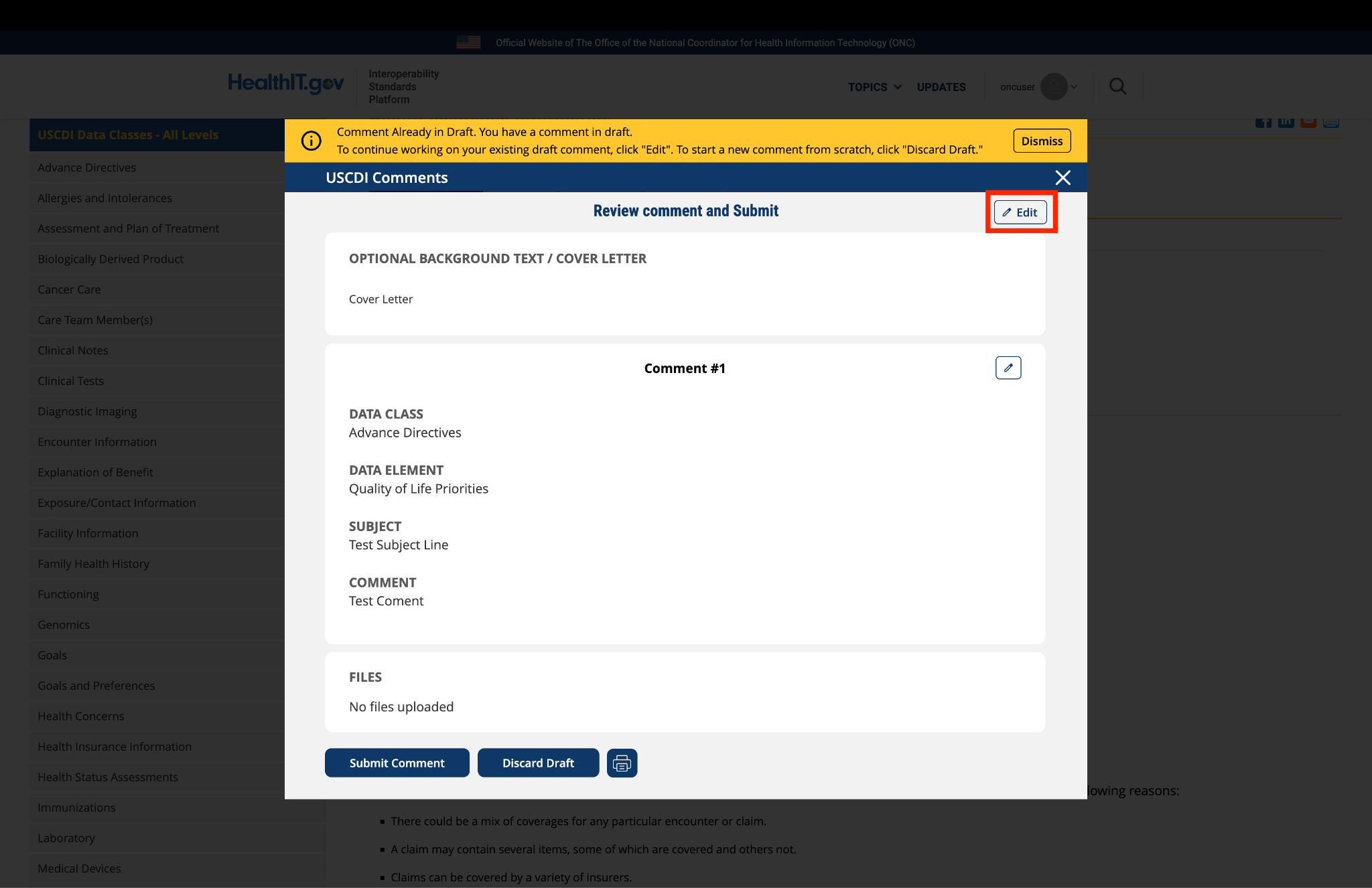
Fig 6 The review screen allows users to verify comment content and make any necessary modifications before final submission.
Submitted by ajohnsondo on
Allegheny Health Network comments on proposed USCDI v2
General Overview: Allegheny Health Network (www.AHN.org), a Highmark Health company, is an integrated healthcare system serving the greater Western Pennsylvania region. The Network is composed of thirteen hospitals, including Allegheny General Hospital, its flagship academic medical center in Pittsburgh. AHN has several nationally recognized programs, over 20,000 employees and nearly 2500 physicians. Highmark Health is one of the largest Blue Cross Blue Shield providers serving patients in multiple states across the US. AHN respectfully submits comments for the USCDI version 2 edition.
Care Team: In a broad sense, a provider of care can be defined as any licensed individual delivering care to patients. As such, our organization lists all independently licensed individuals or appropriately licensed organizations on the "Care Team" only as defined by our technology. We are asking for clarification on the definition of Provider Name as it is related to their licensure status. Additionally, if we presume these are independently licensed providers of care (MD, DO, or others), we would ask the provider identifier be the NPI (National Provider Identifier). Our rationale for this request is that all providers of care on our Care Teams are independently licensed and have a NPI must have their digital address published in their NPPES account.
Encounter Information: There are numerous encounter types for which patients interact with our healthcare system. Many of these encounters include brief non-face to face encounters (e.g., telephone or electronic message) for which defining an encounter diagnosis or even an encounter time may be problematic especially in the case of electronic messaging. As well, some of these encounters may not carry information important to the delivery of care and clutter the information gathering for patients. We believe all appropriate encounters should be included in the data collected. Given the broadening of patient care delivery opportunities today to include a multitude of these types of encounters would be difficult. Additionally, the inclusivity of certain clinical note types in these same encounters carries these same concerns as well. We recommend specific definition around these encounter types where care decisions are made. With this specific definition, we also recommend only the clinical notes generated by these encounters be included in the release to patients for now.
Problems: There will seemingly be a debate on the inclusion of problems vs. diagnoses. We do not wish to enter the debate on this but believe there will be elements which are self-limited diagnoses for which some believe these should not be included on the problem list. These are contrasted with those elements where repeated care is delivered for chronic conditions and should be entered on the patient's problem list. If all diagnoses entered by the providers should be on the problem list, then this should be stated and adhered to so patient's data across multiple encounters, across multiple providers, and across multiple health systems will be useful. Therefore clarification from the committee should include this information.
Diagnostic Imaging: We applaud the creation of a Diagnostic Imaging section similar to the section on laboratory values. The following subsections create the question. We interpreted the definition of Imaging Narrative in the USCDIv1 which is described under the rule as LOINC 18748-4. LOINC 18748-4 is defined as follows: "Diagnostic Imaging Report (DIR) contains a consulting specialist's interpretation of image data. It conveys the interpretation to the referring (ordering) physician and is for use in Radiology, Endoscopy, Cardiology, and other imaging specialties." The USCDIv2 contains the addition of Diagnostic Imaging Report (LOINC search revealed a panel of codes at 72230-6). We are asking for clarification and specifically the difference in the definitions between Diagnostic Imaging Narrative and Diagnostic Imaging Report and the appropriate LOINC coding between these 2 elements. We also find the LOINC code 18782-3, "Radiology Study observation (narrative) which was not mentioned in any of the imaging reporting elements. Please comment.